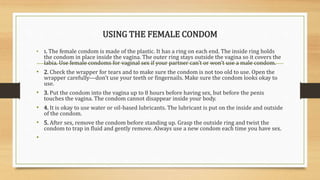
This document provides information on sexual health and family planning. It discusses healthy timing and spacing of pregnancies, different family planning methods, sexually transmitted infections (STIs), and the prevention of STIs and HIV. The key messages are that pregnancy before age 18 or after 35 increases health risks; spacing births at least two years apart benefits mother and child health; and consistent condom use can prevent STIs and HIV transmission. Community health workers are responsible for counseling community members on these topics, making referrals, and empowering people to reduce risky sexual behaviors.