Understanding Sleeping Disorders
Sleep can be regarded as a physiological reversible reduction of conscious awareness.
Sleep is a physical and mental resting rate in which a person becomes relatively inactive
and unaware of the environment.
In essence sleep is a partial detachment from the world, where most external stimuli are
blocked from the senses.
Normal sleep is characterized by a general decrease in body temperature, blood pressure,
breathing rate, and most other bodily functions. In contrast, the human brain never decrease
Inactivity. Studies have shown that the brain is as active during sleep as it is when awake.
Throughout an eight our sleep cycle, a normal adult alternates between two very different
states, Non REM and REN.
It is observed in all mammals, all birds, and may reptiles, amphibians and fish.
3.
Five Stage ofHuman Sleep
Stage 1 NERM Sleep: This Stage occurs while a person is falling a sleep. It represent about 5% of a normal adults sleep time.
Stage 2 NERM Sleep : In this stage, the beginning of “true” sleep), the person’s electroencephalogram (EEG) will show distinctive wave from call sleep spindles
and k complexes about 50% of the sleep time is stage 2 REM sleep.
Stage 3 and 4 NERM Sleep. Also called delta or slow wave sleep these are the deepest level of human sleep and represent 10-20% of sleep time. They usually
occur during the first 30-50% of the sleep period. There is a marked secretion of growth hormone in stage 4
Rem sleep: REM sleep marks up 20% of our sleep time and during this stage we experience vivid dreams. It usually begins about 90 minutes after the person falls
sleep, an important measure called REM latency. It alternates with sleep about every hour and a half throughout the night. REM periods increase in length over
the course of the night.
4.
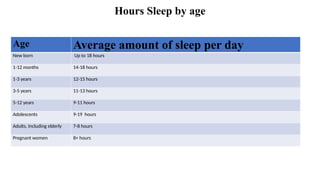
Hours Sleep byage
Age Average amount of sleep per day
New born Up to 18 hours
1-12 months 14-18 hours
1-3 years 12-15 hours
3-5 years 11-13 hours
5-12 years 9-11 hours
Adolescents 9-19 hours
Adults, Including elderly 7-8 hours
Pregnant women 8+ hours
5.
Sleep disorder defined
Sleeping disorders are conditions that affect the quality, timing, and duration of sleep. These
disorders can lead to daytime fatigue, mood disturbances, and cognitive impairment.
A sleeping disorder is a condition that regularly affects the quality, timing, or amount of
sleep, leading to problems with functioning during the day. People with sleep disorders
may have trouble falling asleep, staying asleep, or may feel tired even after getting enough
hours of sleep.
A sleeping disorder is a health problem that makes it hard for a person to get good, restful
sleep. It can cause trouble falling asleep, staying asleep, or feeling rested during the day
Group of syndromes characterized by disturbance in the patients amount of sleep, quality
or timing of sleep, or in behaviours ir physiological conditions associated with sleep.
Understanding the various types of sleeping disorders is essential for effective treatment and
managements
There are about 70 different sleep disorders’
The conditions must be a persistent problem cause the patients significant emotional
distress, and interfere with his or her social or occupational functioning
6.
Predisposing Factor tosleeping disorder
Genetic or familial patterns are thought to play a contributing role in insomnia, primary
hypersomnia, narcolepsy, sleep terror disorder , and sleepwalking
A number of medical conditions as well aging have been implicated in the aetiology of
insomnia.
Psychiatric or environmental conditions, that can contribute to insomnia or hypersomnia
include anxiety, depression, environmental changes, circadian rhythm sleep disturbances,
Puts', and Schizophrenia.
Night terrors may be related to minor neurological abnormalities, particularly in the
temporal lobe.
Episodes of sleepwalking are exacerbated by extreme fatigue and sleep deprivation.
Activities that interfere with 24- hour circadian rhythm of hormonal and neurotransmitter
functioning within the body predispose individual to sleep-wake Schedule disturbances
7.
Primary Sleeping Disorder
Primary sleep disorder are distinguished from those that are not caused by other
mental disorder, Prescription medications, Substance abuse, or medical Conditions.
There are two major Categories of primary sleep disorders are.
Dyssomnias
Parasomnias
Dyssomnias
Primary sleep disorder in which the patients suffers from changes in the amount,
restfulness, and timing of sleep
Insomnia
difficulty infalling asleep or
remaining
asleep that lasts for at least one
month.
can be caused by a traumatic event
related to sleep or bedtime, and it is
often associated with increased
physical or psychological arousal at
Night
People who experience primary
insomnia are often anxious about not
being able to sleep
usually begins when the person is a
young adult or in middle age
Diagnostic criteria for
Primary Insomnia
A. The predominant complaint is difficulty initiating or
maintaining sleep, or nonrestorative sleep, for at least 1
month.
B. The sleep disturbance (or associated daytime fatigue)
causes clinically significant distress or impairment in
social, occupational, or other important areas of
functioning.
C. The sleep disturbance does not occur exclusively
during the course of Narcolepsy, Breathing-Related Sleep
Disorder, Circadian Rhythm Sleep Disorder, or a
Parasomnia.
D. The disturbance does not occur exclusively during the
course of another mental disorder (e.g., Major Depressive
Disorder, Generalized Anxiety Disorder, a Delirium).
E. The disturbance is not due to the direct physiological
effectsof a substance (e.g., a drug of abuse, a medication)
or a general medical condition.
10.
Hypersomnia
a conditionmarked by excessive
sleepiness during normal waking
hours.
The patient has either lengthy
episodes of daytime sleep or
episodes of daytime sleep on a daily
basis even though he or she is
sleeping normally at night.
In some cases, patients with primary
hypersomnia have difficulty waking
in the morning and may appear
confused or angry---condition is
sometimes called sleep drunkenness
and more common in males.
usually affects young adults
between the ages of 15 and 30
Diagnostic criteria for Primary Hypersomnia
The predominant complaint is excessive sleepiness for at
least 1 month (or less if recurrent) as evidenced by either
prolonged sleep episodes or daytime sleep episodes that occur
almost daily.
The excessive sleepiness causes clinically significant distress
or impairment in social, occupational, or other important
areas of functioning.
. The excessive sleepiness is not better accounted for by
Insomnia and does not occur exclusively during the course of
another Sleep Disorder (e.g., Narcolepsy, Breathing-Related
Sleep Disorder, Circadian Rhythm Sleep Disorder, or a
Parasomnia) and cannot be accounted for by an inadequate
amount of sleep.
The disturbance does not occur exclusively during the course
of another mental disorder.
The disturbance is not due to the direct physiological effects
of a substance (e.g., a drug of abuse, a medication) or a
general medical condition.
Specify if: Recurrent: if there are periods of excessive
sleepiness that last at least 3 daysoccurring several times a
year for at least 2 years
11.
Narcolepsy
characterized byrecurrent "sleep attacks" that
the patient cannot fight
The sleep attacks are about 10-20 minutes long.
The patient feels refreshed by the sleep, but
typically feels sleepy again several hours later.
About 40% of patients with narcolepsy have
or have had another mental Disorder
Almost 18% of patients with narcolepsy are 10
years old or younger
Men and women are equally affected.
Narcolepsy
Major symptoms:
Cataplexy is the sudden loss of muscle
tone and stability ("drop attacks")
Hallucinations may occur just before
falling asleep (hypnagogic) or right after
waking up (hypnopompic) and are
associated with an episode of REM
sleep.
Sleep paralysis occurs during the
transition from being asleep to waking
up.
12.
Cont.
Diagnostic criteria forNarcolepsy
Irresistible attacks of refreshing sleep that occur daily over at least 3 months.
The presence of one or both of the following:
cataplexy (i.e., brief episodes of sudden bilateral loss of muscle tone, most often in association with intense
emotion)
recurrent intrusions of elements of rapid eye movement (REM) sleep into the transition between sleep and
wakefulness, as manifested by either hypnopompic or hypnagogic hallucinations or sleep paralysis at the beginning
or end of sleep episodes
The disturbance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or
another general medical condition.
13.
Breathing-related Sleep Disorders
syndromes in which the patient's sleep is interrupted by problems with his or her breathing
4 types of breathing-related sleep disorders:
Obstructive sleep apnea syndrome. This is the most common form of breathing-related sleep
disorder, marked by episodes of blockage in the upper airway during sleep. It is found primarily in
obese people. Patients with this disorder typically alternate between periods of snoring or gasping
(when their air way is partly open) and periods of silence (when their airway is blocked). Very loud
snoring is a clue to this disorder.
Central sleep apnea syndrome. This disorder is primarily found in elderly patients with heart or
neurological conditions that affect their ability to breathe properly. It is not associated with airway
blockage and may be related to brain disease.
Central alveolar hypoventilation syndrome. This disorder isfound most often in extremely obese
people. The patient's
airway is not blocked, but his or her blood oxygen level is too low.
Mixed-type sleep apnea syndrome. This disorder combines symptoms of both obstructive and
central sleep apnea.
14.
Cont..
Diagnostic criteria forBreathing-Related Sleep Disorder
Sleep disruption, leading to excessive sleepiness or insomnia, that is judged to be due to a sleep-related
breathing condition (e.g., obstructive or central sleep apnea syndrome or central alveolar hypoventilation
syndrome).
The disturbance is not better accounted for by another mental disorder and is not due to the direct physiological
effects of a substance (e.g., a drug of abuse, a medication) or another general medical condition (other than a
breathing-related disorder).
Coding note: Also code sleep-related breathing disorder on Axis III.
15.
Circadian Rhythm Sleep
Disorders
Results from a discrepancy between the
person's daily sleep/wake patterns and
demands of social activities, shift work, or
travel.
Examples include delayed sleep phase
disorder and shift work disorder.
Treatment typically focuses on re-
aligning the sleep schedule with natural
light patterns.
16.
Cont…
Types of CircadianRhythm Sleep Disorders
Jet lag
sleepiness and alertness that occur at an inappropriate time of day relative to local time, occurring after repeated travel across more
than one time zone
Shift work
insomnia during the major sleep period or excessive sleepiness during the major awake period associated with night shift work or frequently changing
shift.
work Non-24-hour sleep-wake syndrome
• rare and chronic circadian rhythm sleep disorder.
• "a chronic steady pattern comprising one- to two- hour daily delays in sleep onset and wake times in an individual living in society.“
• The pattern of delay persists literally "around the clock," typically taking a few weeks to complete one cycle.
• It affects less than 0.05% of the population (fewer than 1 in 2000 people), which means that it is classified as a "rare disease.
17.
Restless Legs Syndrome
(RLS)
RLS is a neurological disorder causing uncomfortable
sensations in the legs, often accompanied by an urge to
move them.
Symptoms typically worsen in the evening or during
periods of inactivity.
Treatment may include medications, lifestyle adjustments,
and addressing underlying conditions.
18.
PARASOMNIAS
primary sleep disordersin which the
patient's behavior is affected by
specific sleep stages or transitions
between sleeping and waking. They are
sometimes described as disorders of
physiological arousal during sleep.
There are the types of Parasomnias
Nightmare Disorder
Sleep Terror Disorder
Sleeping Walking Disorder
Nightmare Disorder
parasomnia in which there patient is repeatedly
awakened from sleep by frightening dreams and
is fully alert on awakening.
Approximately 10-50% of children between
three and five years old have nightmares.
They occur during REM sleep, usually in the
second half of the night
The child is usually able to remember the
content of the nightmare and may be afraid to go
back to sleep.
More females than males have this disorder, but
it is not known whether the sex difference
reflects a difference in occurrence or a difference
in reporting.
Nightmare disorder is most likely to occur in
children or adults under severe or traumatic
stress.
19.
Cont..
Diagnostic criteria forNightmare Disorder
Repeated awakenings from the major sleep period or naps with detailed recall of extended and extremely frightening dreams, usually
involving threats to survival, security, or self- esteem. The awakenings generally occur during the second Half of the sleep period.
On awakening from the frightening dreams, the person rapidly becomes oriented and alert (in contrast to the confusion and disorientation
seen in Sleep Terror Disorder and some forms of epilepsy).
The dream experience, or the sleep disturbance resulting from the awakening, causes clinically significant distress or impairment in
social, occupational, or other important areas of functioning.
The nightmares do not occur exclusively during the course of another mental disorder (e.g., a Delirium, Posttraumatic Stress Disorder)
and are not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition.
20.
Sleep Terror Disorder
Sleep Terror Disorder is a parasomnia in which the
patient awakens screaming or crying.
The patient also has physical signs of arousal,
like sweating, shaking, etc.
It is sometimes referred to as pavor nocturnus.
Unlike nightmares, sleep terrors typically occur
in stage 3 or stage 4 NREM sleep during the first
third of the night.
The patient may be confused or disoriented for
several minutes and cannot recall the content
of the dream.
He or she may fall asleep again and not
remember the episode the next morning.
Sleep terror disorder is most common in
children four to 12 years old and is outgrown in
adolescence.
It affects about 3% of children.
Fewer than 1% of adults have the disorder. I
in adults, it usually begins between the ages of
20 and 30.
In children, more males than females have the
disorder. In adults, men and women are equally
affected.
Diagnostic criteria for Sleep
Terror Disorder
Recurrent episodes of abrupt awakening from sleep,
usually occurring during the first third of the major
sleep episode and beginning with a panicky scream.
Intense fear and signs of autonomic arousal, such as
tachycardia, rapid breathing, and sweating, during
each episode.
Relative unresponsiveness to efforts of others to
comfort the person during the episode.
No detailed dream is recalled and there is amnesia
for the episode.
The episodes cause clinically significant distress or
impairment in social, occupational, or other
important areas of functioning.
The disturbance is not due to the direct physiological
effects of a substance (e.g., a drug of abuse, a
medication) or a general medical condition.
21.
Periodic Limb MovementDisorder
affects people only during sleep.
The condition is characterized by behavior ranging from shallow,
continual movement of the ankle or toes, to wild and strenuous kicking
and flailing of the legs and arms.
Furthermore, abdominal, oral, and nasal movement sometimes
accompanies PLMD.
Movement of the legs is more typical than movement of the arms in
cases of PLMD.
Movements typically occur for 0.5 to 10 seconds, in intervals
separated by five to 90 seconds.
A formal diagnosis of nocturnal myoclonus requires three periods
during the night, lasting from a few minutes to an hour or more, each
containing at least 30 movements followed by partial arousal or
awakening. (ASDC 1979)
These limb movements
22.
Sleep walking disorder
sometimes called somnambulism
occurs when the patient is capable of complex
movements during sleep, including walking.
Like sleep terror disorder, sleepwalking occurs
during stage 3 and stage 4 NREM sleep during
the first part of the night.
If the patient is awakened during a
sleepwalking episode, he or she may be
disoriented and have no memory of the
behavior.
In addition to walking around, patients with
sleepwalking disorder have been reported to eat,
use the bathroom, unlock doors, or talk to
others. It is estimated that 10-30% of children
have at least one episode of sleepwalking.
However, only 1-5% meet the criteria for
sleepwalking disorder.
The disorder is most common in children eight
to 12 years old.
It is unusual for sleepwalking to occur for the
first time
in adults.
Diagnostic criteria for Sleepwalking
Disorder
Repeated episodes of rising from bed during sleep and
walking about, usually occurring during the first third of
the major sleep episode.
While sleepwalking, the person has a blank, staring face,
is relatively unresponsive to the efforts of others to
communicate with him or her, and can be awakened only
with great difficulty.
On awakening (either from the sleepwalking episode or
the next morning), the person has amnesia for the
episode.
Within several minutes after awakening from the
sleepwalking episode, there is no impairment of mental
activity or behavior (although there may initially be a
short period of confusion or disorientation).
The sleepwalking causes clinically significant distress or
impairment in social, occupational, or other important areas
of functioning.
The disturbance is not due to the direct physiological
effects of a substance (e.g., a drug of abuse, a
medication) or a general medical condition.
23.
symptoms of sleepingdisorders
Trouble Falling Asleep
You lie in bed for a long time but can't sleep
Waking Up Often at Night
You wake up many times during the night and find it hard to go back to sleep.
Waking Up Too Early
You wake up much earlier than you want and can't fall asleep again.
Still Feeling Tired After Sleep
Even after sleeping, you don’t feel refreshed or energetic.
Daytime Sleepiness
You feel sleepy, drowsy, or tired during the day, even after a full night’s sleep.
Difficulty Concentrating or Forgetfulness
You find it hard to focus, remember things, or stay alert.
Irritability or Mood Swings
You feel more annoyed, sad, or emotional than usual.
Falling Asleep While Driving or Working
Feeling so sleepy that you doze off in dangerous situations.
Snoring or Choking During Sleep
Loud snoring or gasping for air while sleeping (often seen in sleep apnea).
24.
Causes of SleepingDisorders
Sleeping disorders can stem from various factors, including medical,
psychological, and environmental influences.
Stress, anxiety, and depression are significant contributors to insomnia and
other sleep issues.
Physical health problems, such as heart disease or chronic pain, can also
disrupt sleep.
Some other Causes of Sleeping Disorders
Poor Sleep Habits
Medical Conditions
Medications
Neurological Disorders
Substance Abuse
Genetics
Hormonal Changes
Eating Late at Night
Lack of Physical Activity
25.
Effects of SleepingDisorder
Poor Concentration and Memory
You may forget things easily or find it hard to focus. Tasks that require thinking or decision-making
feel more difficult.
Mood Changes
You may feel more irritated, anxious, or sad. Small things can upset you more than usually
Weak Immune System
Your body becomes less able to fight off colds, flu, and other infections. You get sick more often.
Heart Problems
Sleep disorders can lead to high blood pressure, heart disease, or stroke. Your heart needs rest to stay
healthy
Weight Gain
Lack of sleep affects hormones that control hunger. You may feel hungrier and crave unhealthy food.
Accidents and Injuries
Sleepiness slows your reaction time. This increases the risk of accidents while driving or working
Poor Performance at School or Work
You may have trouble finishing tasks or meeting deadlines. Grades or job performance may drop.
Mental Health Issues
Long-term sleep problems can lead to anxiety, depression, or other mental health conditions
26.
Treatment of SleepingDisorder
Cognitive Behavioral Therapy (CBT)
A type of talk therapy that helps you change negative thoughts and habits about sleep.
Very effective for insomnia.
Medications (Sleep Aids)
Doctors may prescribe sleeping pills or other medications for short-term use. These
should only be used under a doctor’s advice.
Lifestyle Changes
Going to bed and waking up at the same time every day Avoiding naps during the day.
Limiting screen time before bed.
Relaxation Techniques
Deep breathing, meditation, or gentle yoga can help calm your mind before sleeping.
Improving Sleep Environment
Keep your bedroom dark, quiet, and cool. Use a comfortable mattress and pillow.
Avoiding Caffeine, Alcohol, and Heavy Meals Before Bed
These can disturb your sleep or make it hard to fall asleep.
Treatment of Underlying Medical Conditions
If your sleep problems are caused by conditions like asthma, depression, or chronic pain,
treating those first can improve sleep.
Sleep Devices (for sleep apnea)
Devices like CPAP machines help people with sleep apnea breathe properly during sleep.
27.
Conclusion
Sleeping disorderssignificantly impact physical and mental health, reducing overall quality
of life.
Common types include insomnia, sleep apnea, narcolepsy, and restless legs syndrome.
They can be caused by stress, medical conditions, lifestyle habits, or genetic factors.
Early diagnosis and treatment are crucial to prevent long-term health consequences.
Lifestyle changes, therapy, and in some cases, medications can effectively manage
symptoms.
Raising awareness and promoting good sleep hygiene are essential for prevention and
management.
Continued research and support are needed to improve treatment outcomes and public
understanding
Understanding sleeping disorders is crucial for improving health and well-being.
A multi-faceted approach that includes lifestyle changes, therapy, and, if necessary,
medication is often most effective.
Awareness and education can empower individuals to seek help and enhance their sleep
quality.
28.
References
Data sourced fromNIH, CDC, American Academy of Sleep Medicine, and
peer-reviewed journals.
Healthcare costs estimated by Sleep Research Society and National
Sleep Foundation.
Statistics on prevalence and impact based on recent US studies.