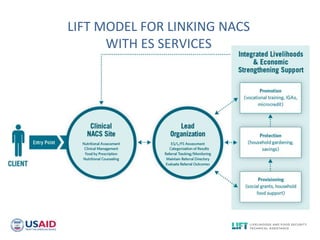
The document provides an overview of the LIFT project, which aims to improve linkages between HIV/AIDS clinical services and economic strengthening programs. It discusses research conducted in Ethiopia and Namibia to identify challenges and promising practices around referral systems. Key findings include the importance of designated case managers, community coordination committees, and formalizing bi-directional referral processes between clinics and community organizations. The LIFT model proposes strengthening existing economic strengthening services, identifying gaps, and engaging the private sector to improve sustainable employment for clients of HIV clinical programs.