Dr Umesh KumarMaurya 1
Thyroid Hormones and Thyroid Inhibitors
Presenter: Dr Umesh Kumar Maurya (JR-1)
Moderator: Dr Ashish Dixit (SR)
Peer support: Dr Naveen Maurya (JR-1)
Department of Pharmacology and Therapeutics
King George Medical University Lucknow (UP), India
Email id - drumeshkgmu@gmail.com
20/05/2025
2.
Dr Umesh KumarMaurya 2
Contents
• Introduction
• Thyroid hormones and their biosynthesis
• Classification of thyroid inhibitors
• Therapeutic uses of antithyroid drugs
• Summary
20/05/2025
3.
Dr Umesh KumarMaurya 3
Specific learning objectives
By end of this teaching learning session co-learners will be able to:
• Describe the synthesis of thyroid hormones
• Explain clinical features of hypothyroidism and hyperthyroidism
• Explain the classification of thyroid inhibitors
• Enumerate uses of antithyroid drugs
20/05/2025
4.
Dr Umesh KumarMaurya 4
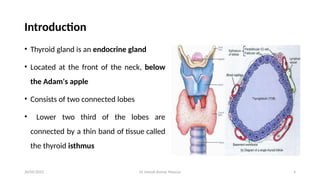
Introduction
• Thyroid gland is an endocrine gland
• Located at the front of the neck, below
the Adam's apple
• Consists of two connected lobes
• Lower two third of the lobes are
connected by a thin band of tissue called
the thyroid isthmus
20/05/2025
5.
Dr Umesh KumarMaurya 5
Thyroid hormones
Thyroid gland secretes 3 hormones
1. T4 - 3,5,3’,5’ tetra-iodothyronine or thyroxine
2. T3 - 3,5,3’ tri-iodothyronine
3. Calcitonin is produced by interfollicular ‘C’ cells
Both T4 and T3 are iodine containing derivatives of thyronine which is a
condensation product of 2 molecules of tyrosine
produced by thyroid
follicles
20/05/2025
6.
Dr Umesh KumarMaurya 6
Biosynthesis
Synthesis, storage and release of T4 and T3 involves the following processes:
1. Iodide uptake
2. Oxidation, Organification and Coupling
3. Storage and release
4. Peripheral conversion of T4 to T3
20/05/2025
7.
Dr Umesh KumarMaurya 7
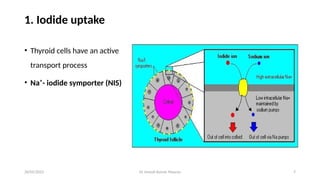
1. Iodide uptake
• Thyroid cells have an active
transport process
• Na⁺- iodide symporter (NIS)
20/05/2025
8.
Dr Umesh KumarMaurya 8
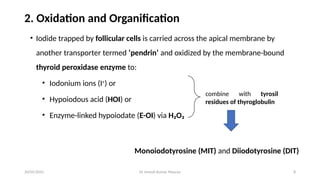
2. Oxidation and Organification
• Iodide trapped by follicular cells is carried across the apical membrane by
another transporter termed ‘pendrin’ and oxidized by the membrane-bound
thyroid peroxidase enzyme to:
• Iodonium ions (I+
) or
• Hypoiodous acid (HOI) or
• Enzyme-linked hypoiodate (E-OI) via H₂O₂
Monoiodotyrosine (MIT) and Diiodotyrosine (DIT)
combine with tyrosil
residues of thyroglobulin
20/05/2025
9.
Dr Umesh KumarMaurya 9
3. Coupling
• Pair of iodinated tyrosil residues couple together to form T3 and T4
• Normally more T₄ is formed than T₃
• Oxidation of iodide and coupling are both stimulated by TSH
20/05/2025
10.
Dr Umesh KumarMaurya 10
4. Storage and Release
• MIT, DIT, T₃ and T₄ – all attached to thyroglobulin and stored in the colloid
• Taken up by follicular cells by the process of endocytosis and broken down
by lysosomal proteases
• T₃ and T₄ so released is secreted into circulation
• MIT and DIT residues are deiodinated and iodide released is reutilized
• Normal human thyroid secretes 60–90 μg of T₄ and 10–30 μg of T₃ daily
20/05/2025
11.
Dr Umesh KumarMaurya 11
5. Peripheral Conversion of T₄ to T₃
• Peripheral tissues (liver and kidney) convert T₄ to T₃
• T4 to T3 conversion is carried out by iodothyronine deiodinase
• Target tissues take up T₃ from circulation for their metabolic need
• Equal amounts of T₃ (3,5,3’ triiodothyronine, normal T3:active) and rT₃ (3,3’,5’
triiodothyronine, reverse T3: inactive)are produced in the peripheral tissues
20/05/2025
12.
Dr Umesh KumarMaurya 12
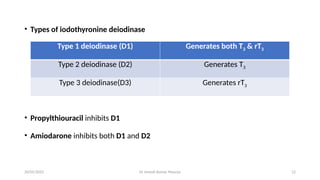
• Types of iodothyronine deiodinase
• Propylthiouracil inhibits D1
• Amiodarone inhibits both D1 and D2
Type 1 deiodinase (D1) Generates both T3 & rT3
Type 2 deiodinase (D2) Generates T3
Type 3 deiodinase(D3) Generates rT3
20/05/2025
13.
Dr Umesh KumarMaurya 13
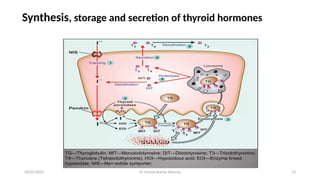
Synthesis, storage and secretion of thyroid hormones
20/05/2025
14.
Dr Umesh KumarMaurya 14
Transport, metabolism and excretion
• Only 0.03-0.08% of T₄ and 0.2-0.5% of T₃ are in free form
• Main plasma proteins are – TBG (Thyroxine Binding Globulin), TBP (Thyroxine
Binding Prealbumin) and Albumin
• Metabolism: mainly in liver and kidneys by deiodination and conjugation
• Conjugated products excreted by bile – enterohepatic circulation into urine
• Plasma t½ of T₄ is 6-7 days, while that of T₃ is 1-2 days
20/05/2025
15.
Dr Umesh KumarMaurya 15
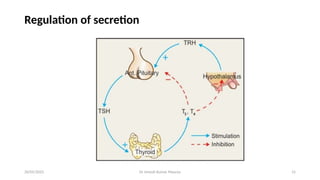
Regulation of secretion
20/05/2025
16.
Dr Umesh KumarMaurya 16
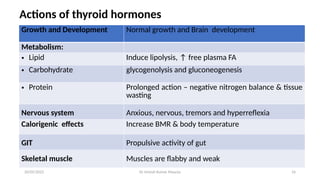
Actions of thyroid hormones
Growth and Development Normal growth and Brain development
Metabolism:
• Lipid Induce lipolysis, ↑ free plasma FA
• Carbohydrate glycogenolysis and gluconeogenesis
• Protein Prolonged action – negative nitrogen balance & tissue
wasting
Nervous system Anxious, nervous, tremors and hyperreflexia
Calorigenic effects Increase BMR & body temperature
GIT Propulsive activity of gut
Skeletal muscle Muscles are flabby and weak
20/05/2025
17.
Dr Umesh KumarMaurya 17
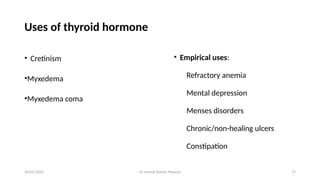
Uses of thyroid hormone
• Cretinism
•Myxedema
•Myxedema coma
• Empirical uses:
Refractory anemia
Mental depression
Menses disorders
Chronic/non-healing ulcers
Constipation
20/05/2025
18.
Dr Umesh KumarMaurya 18
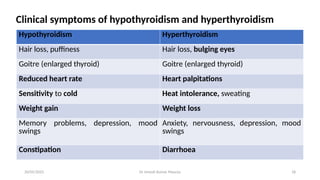
Clinical symptoms of hypothyroidism and hyperthyroidism
Hypothyroidism Hyperthyroidism
Hair loss, puffiness Hair loss, bulging eyes
Goitre (enlarged thyroid) Goitre (enlarged thyroid)
Reduced heart rate Heart palpitations
Sensitivity to cold Heat intolerance, sweating
Weight gain Weight loss
Memory problems, depression, mood
swings
Anxiety, nervousness, depression, mood
swings
Constipation Diarrhoea
20/05/2025
19.
Dr Umesh KumarMaurya 19
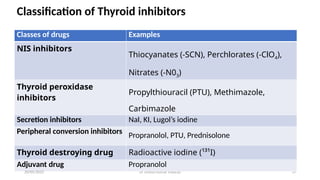
Classification of Thyroid inhibitors
Classes of drugs Examples
NIS inhibitors
Thiocyanates (-SCN), Perchlorates (-ClO4),
Nitrates (-N03)
Thyroid peroxidase
inhibitors
Propylthiouracil (PTU), Methimazole,
Carbimazole
Secretion inhibitors NaI, KI, Lugol’s iodine
Peripheral conversion inhibitors Propranolol, PTU, Prednisolone
Thyroid destroying drug Radioactive iodine (¹³¹I)
Adjuvant drug Propranolol
20/05/2025
20.
Dr Umesh KumarMaurya 20
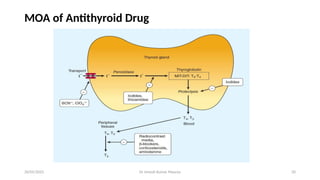
MOA of Antithyroid Drug
20/05/2025
21.
Dr Umesh KumarMaurya 21
NIS inhibitors
• Block uptake of iodide
• Highly toxic effects
• Cabbage is a rich source of Thiocyanate [Goitrogen]
20/05/2025
22.
Dr Umesh KumarMaurya 22
Thyroid peroxidase inhibitors / Antithyroid drugs
• Antithyroid drugs bind to the thyroid peroxidase and prevent oxidation of
iodide/iodotyrosyl residues, thereby:
(i) Inhibit iodination of tyrosine residues in thyroglobulin
(ii) Inhibit coupling of iodotyrosine residues to form T3 and T4
• Propylthiouracil also inhibits peripheral conversion of T4 to T3 by D1 type of 5’
deiodinase
20/05/2025
23.
Dr Umesh KumarMaurya 23
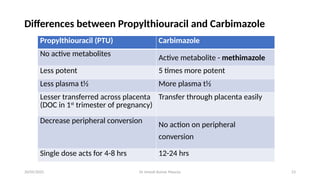
Differences between Propylthiouracil and Carbimazole
Propylthiouracil (PTU) Carbimazole
No active metabolites
Active metabolite - methimazole
Less potent 5 times more potent
Less plasma t½ More plasma t½
Lesser transferred across placenta
(DOC in 1st
trimester of pregnancy)
Transfer through placenta easily
Decrease peripheral conversion No action on peripheral
conversion
Single dose acts for 4-8 hrs 12-24 hrs
20/05/2025
24.
Dr Umesh KumarMaurya 24
Uses of antithyroid drugs
• PTU is DOC in first trimester of pregnancy
• Carbimazole/methimazole is used in second and third trimester
• Long term treatment of thyrotoxicosis
• Thyrotoxic crisis: Propylthiouracil is used along with iodide and propranolol
20/05/2025
25.
Dr Umesh KumarMaurya 25
Secretion inhibitors
• Fastest acting antithyroid drugs
• Excess iodide inhibits its own transport into thyroid cells by inhibiting NIS and
also inhibits iodination of tyrosine residues
• Attenuates TSH stimulation
20/05/2025
26.
Dr Umesh KumarMaurya 26
Uses
• Preoperative preparation before thyroidectomy and thyroid storm
• Prophylaxis of endemic goiter
Adverse effects
• Acute reaction: swelling of lips, eyelids, angioedema of larynx, fever joint pain,
petechial hemorrhages, thrombocytopenia, lymphadenopathy
• Chronic overdose (iodism): Inflammation of mucous membranes, salivation,
blurring sensation in mouth, headache, rashes, GI symptoms etc.
20/05/2025
27.
Dr Umesh KumarMaurya 27
Radioactive iodine
• 131
I physical half life: 8 days
• Emits s (penetrate only 0.5-2mm of tissues)
• Radioactive iodine is administered as sodium salt of 131
I dissolved in water and
taken orally
• Slow acting, cause local soreness in neck
• Incidence of hypothyroidism high
20/05/2025
28.
Dr Umesh KumarMaurya 28
Advantages
1. Treatment with 131
I is simple, conventionally given on outpatient basis and inexpensive
2. No surgical risk, scar or injury to parathyroid glands & recurrent nerves
3. Once hyperthyroidism is controlled, cure is permanent
Disadvantages
1. Hypothyroidism
2. Long latent period of response
3. Contraindicated during pregnancy
20/05/2025
Dr Umesh KumarMaurya 30
Treatment
• Hospitalization
• Propranolol 1-2 mg slow I.V. followed by 40 -80 mg oral 6 hourly
• Propylthiouracil 200-300 oral 6 hourly
• Oral iodides to inhibit the release of thyroid hormones- sodium ipodate inhibits
peripheral conversion of T4 to T3
• Hydrocortisone 100mg I.V. 8 hourly followed by oral prednisolone
20/05/2025
31.
Dr Umesh KumarMaurya 31
Summary
• Thyroid gland secretes 3 hormones T3, T4 and calcitonin
• Biosynthesis includes Iodide uptake or trapping, oxidation, organification,
coupling, storage, release and peripheral conversion of T4 to T3
• NIS inhibitors, Thyroid peroxidase inhibitors, Secretion inhibitors, Peripheral
conversion inhibitors, Radioactive iodine 131
I are thyroid inhibitors
• They are used to treat hyperthyroidism and prepare patients for thyroid surgery
• Radioactive iodine (¹³¹I) treats hyperthyroidism by selectively destroying
overactive thyroid tissue through localized beta radiation
20/05/2025
32.
Dr Umesh KumarMaurya 32
References
• Tripathi KD. Drugs for Cough and Bronchial Asthma. In: Essentials of Medical
Pharmacology. 9th
ed. New Delhi: Jaypee Brothers Medical Publishers; 2019
• Ritter, J. M., Flower, R. J., Henderson, G., Loke, Y. K., MacEwan, D., Robinson, E., &
Fullerton, J. (2023). Rang & Dale’s Pharmacology E-Book: Rang & Dale’s Pharmacology E-
Book. Elsevier Health Sciences
• Goodman, L., Gilman, A., Brunton, L., Lazo, J. and Parker, K. Goodman & Gilman's the
pharmacological basis of therapeutics, New York: McGraw-Hill. 2006
20/05/2025
33.
Dr Umesh KumarMaurya 33
Specific learning objectives achieved
By end of this teaching learning session co-learners are now able to:
• Describe the synthesis of thyroid hormone
• Explain clinical features of hypothyroidism and hyperthyroidism
• Explain the classification of thyroid inhibitors
• Enumerate uses of antithyroid drugs
20/05/2025
Dr Umesh KumarMaurya 35
Questions
1. What are the steps of biosynthesis of thyroid hormones?
2. What are the clinical features of hypothyroidism?
3. What are the clinical features of hyperthyroidism?
4. Describe the classification of thyroid inhibitors
5. Differences between propylthiouracil and carbimazole
20/05/2025




![Dr Umesh Kumar Maurya 21
NIS inhibitors
• Block uptake of iodide
• Highly toxic effects
• Cabbage is a rich source of Thiocyanate [Goitrogen]
20/05/2025](https://image.slidesharecdn.com/thyroid-1-250521125521-f742a130/85/thyroid-hormones-and-thyroid-inhibitors-21-320.jpg)