The document provides an extensive overview of the thyroid gland, including its anatomy, development, physiology, and associated conditions such as hyperthyroidism and hypothyroidism. It discusses the gland's structure, blood supply, nerve relations, common symptoms, diagnosis, and treatment options, including surgical and medical interventions for various thyroid disorders. Additionally, congenital anomalies and their management are addressed, emphasizing the importance of understanding thyroid function and pathology in clinical practice.

![Nerves relation to thyroid
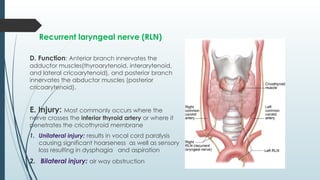
🠶 Recurrent laryngeal nerve (RLN)
branch of the vagus (cranial nerve [CN] X)
that runs in the tracheoesophageal groove at the
posteromedial aspect of the thyroid
A. On the right: RLN recurs round the subclavian
artery and runs an oblique course, crossing the
inferior thyroid artery before entering the TE
groove.
B. On the left : RLN recurs round the ligmentum
arteriosum in the mediastinum and runs course
parallel to the TE groove.
RLN divides at variable locations into an anterior
branch and posterior branch.](https://image.slidesharecdn.com/thyroidgland6yearfinal2024-241117160250-f61f7c6f/85/thyroid-gland-6-year-final-2024-ppt-ddx-13-320.jpg)



























![Thyroid_Gland_Introduction&embryology[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidglandintroductionembryology1-250604192159-6ad15b98-thumbnail.jpg?width=640&height=640&fit=bounds)