
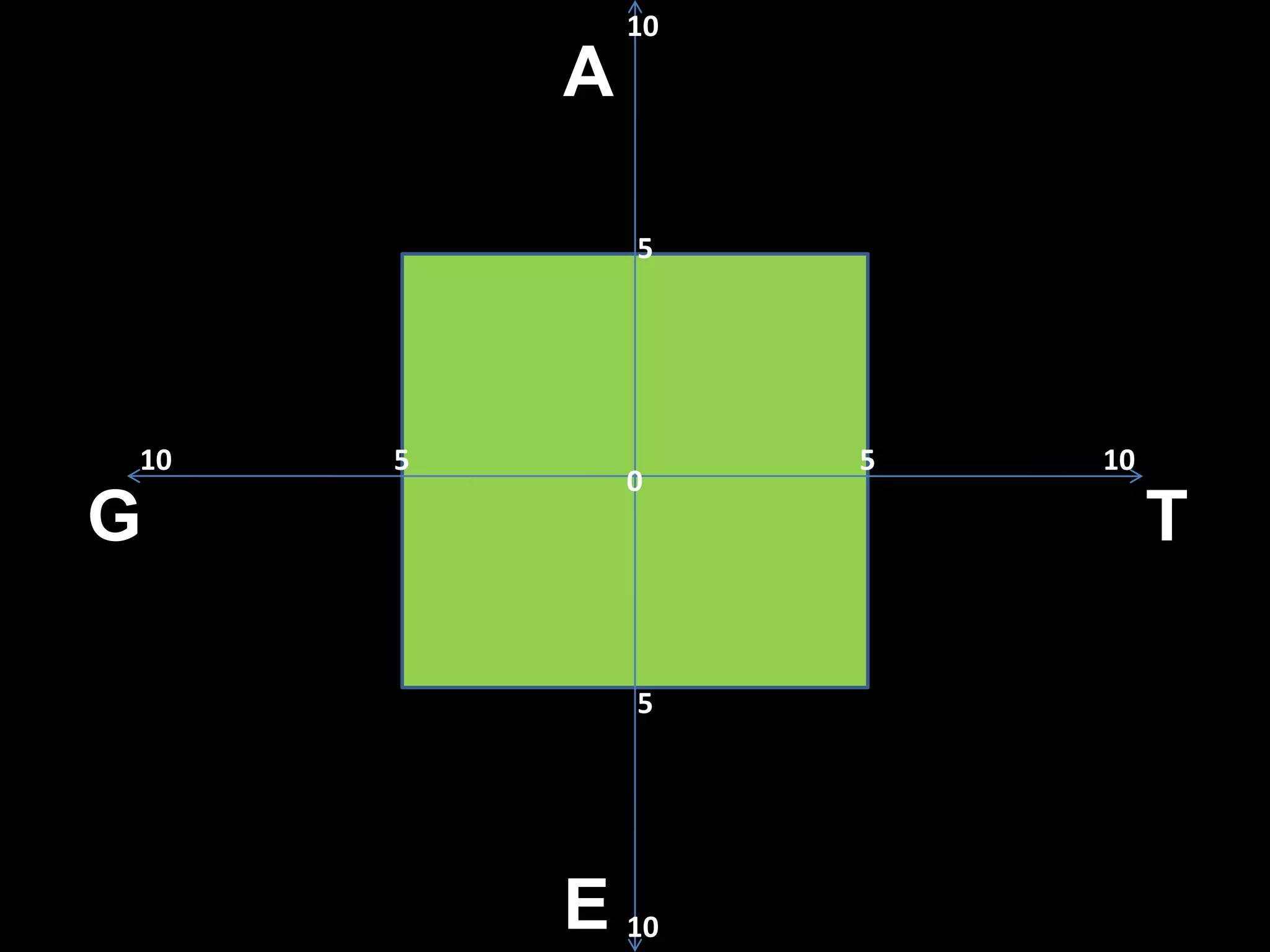
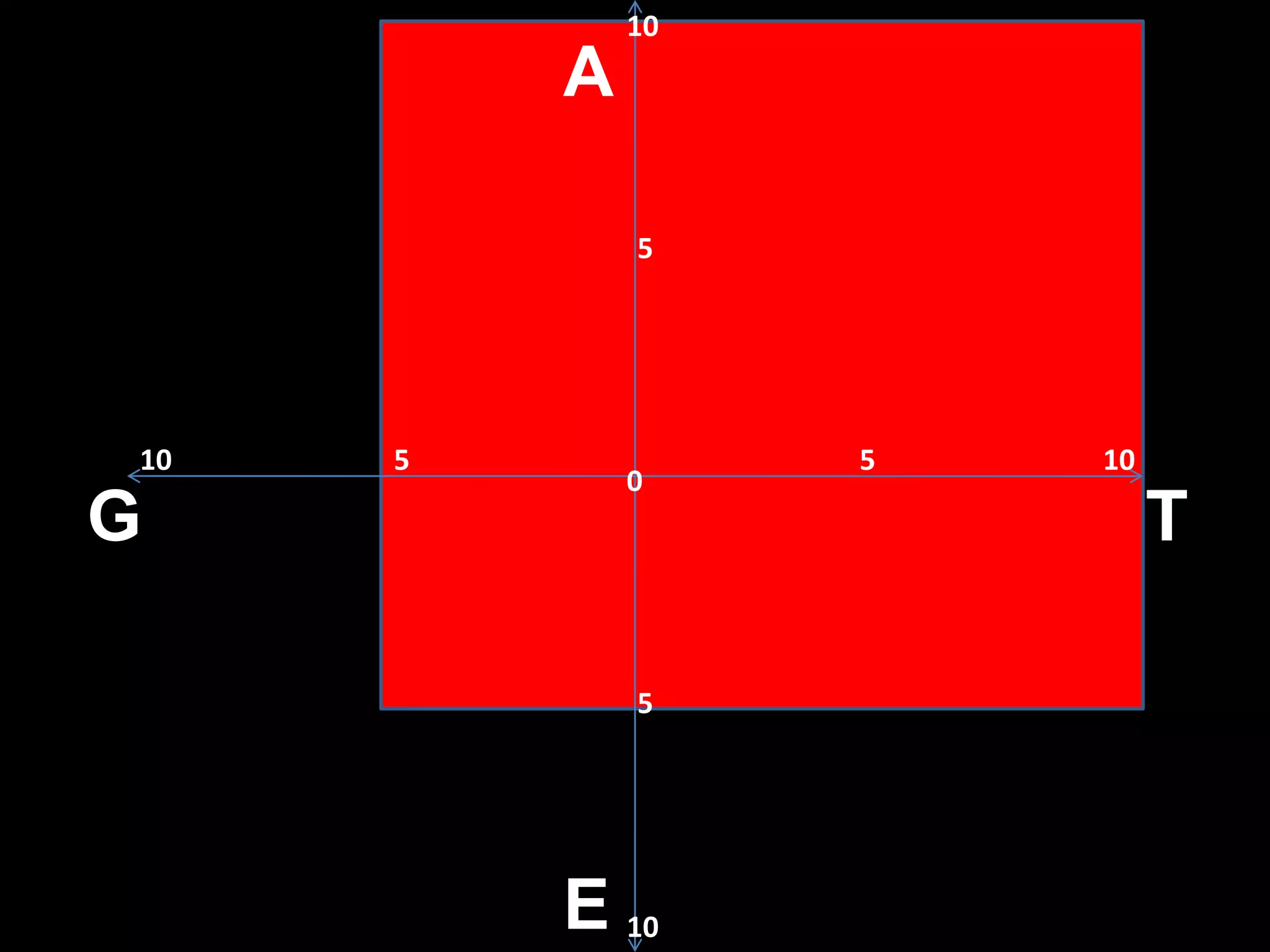
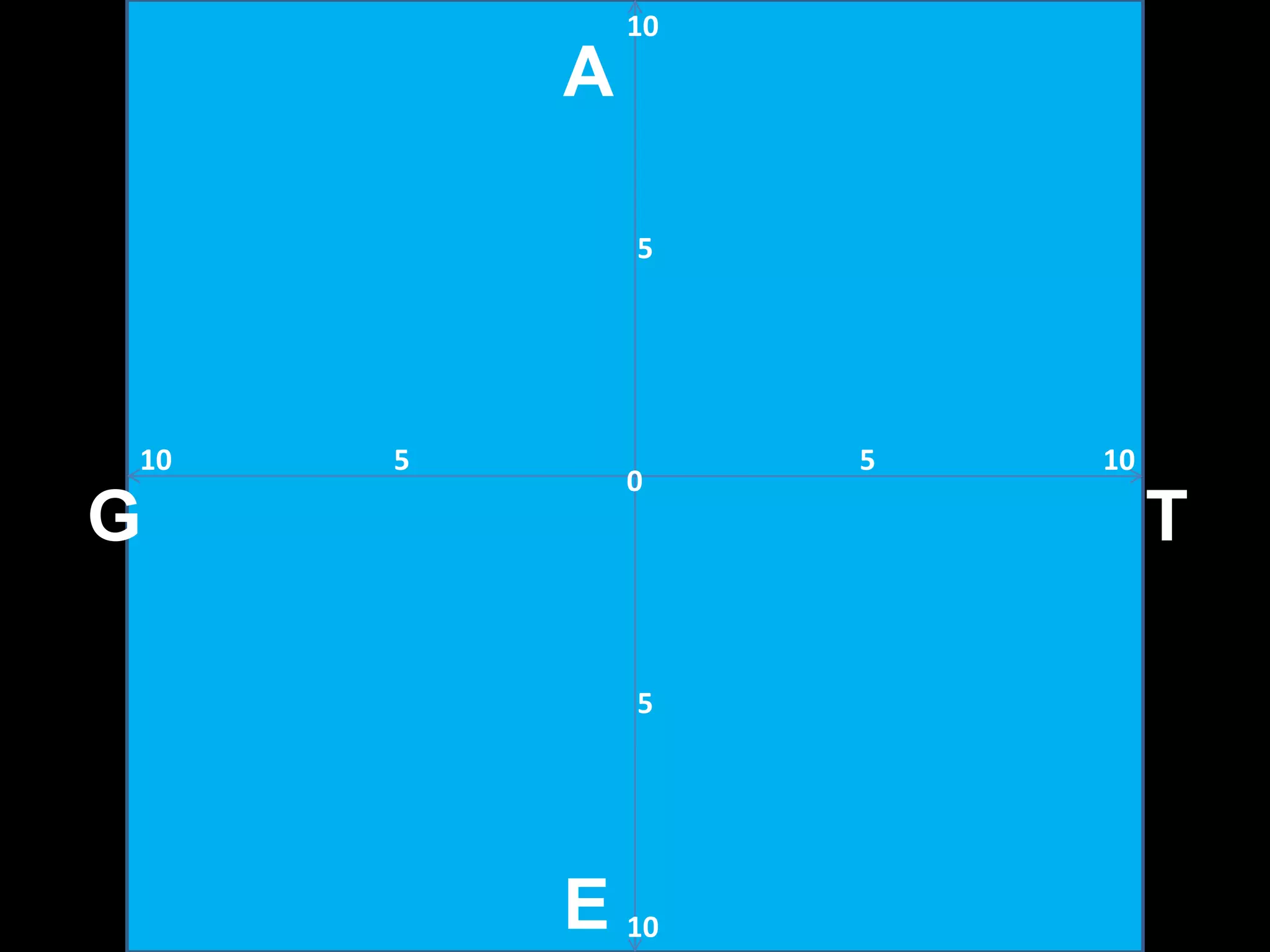
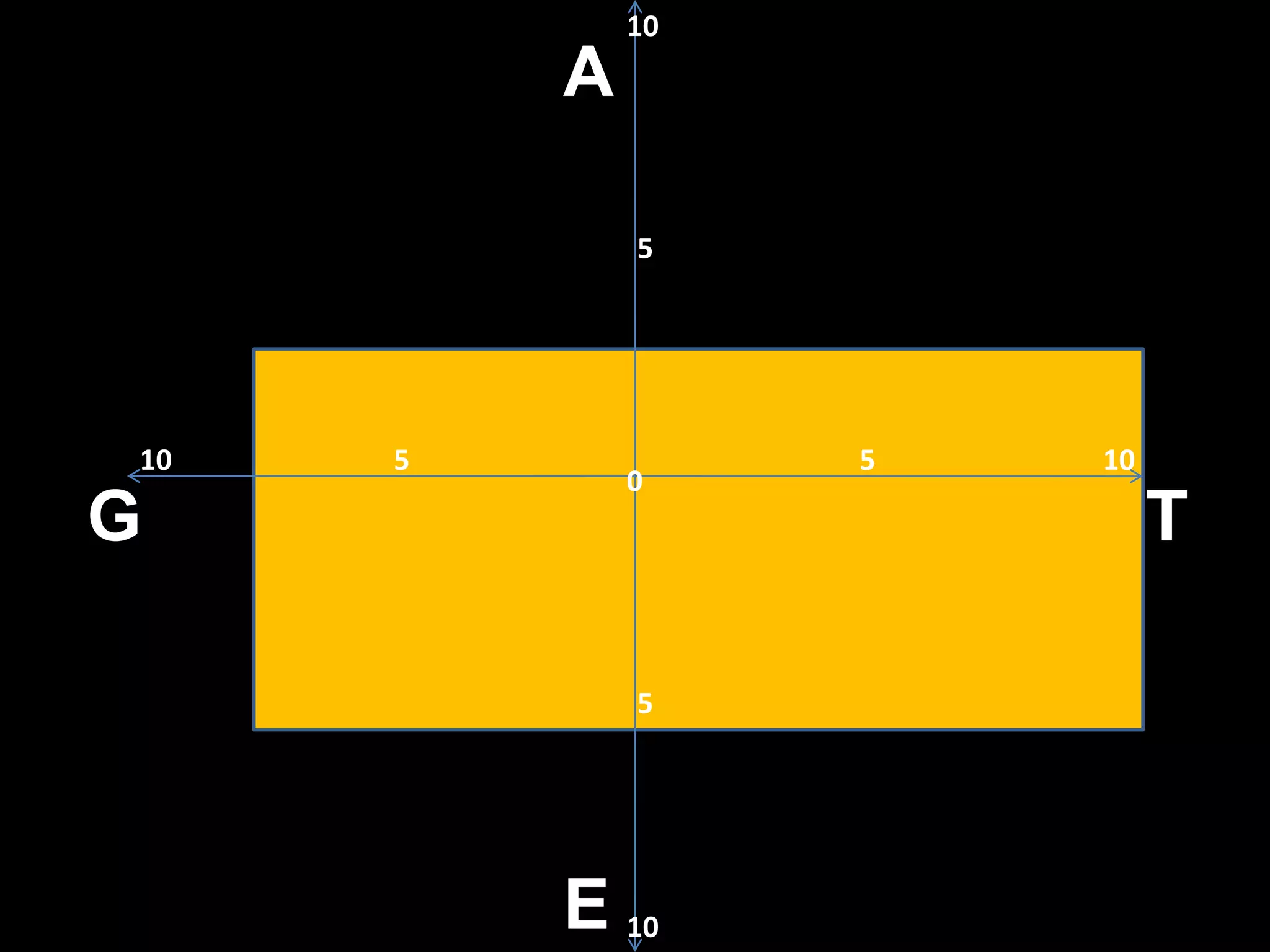

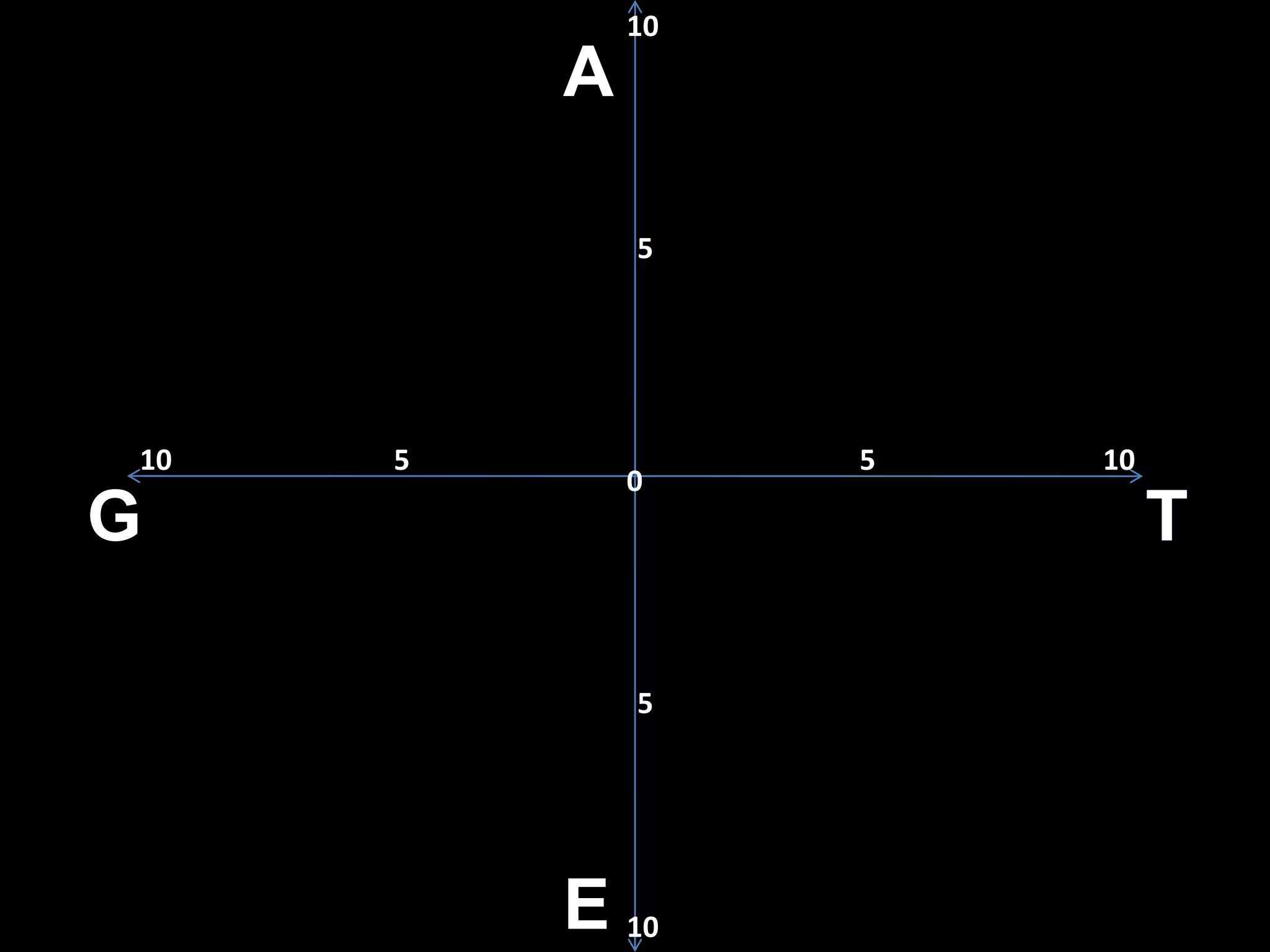

The Gate Model is a comprehensive approach to assessing and treating addictions, developed over 20 years of clinical practice and focusing on the multidimensional aspects of addiction including trauma, genetics, and environmental factors. It provides a framework for evaluating an individual's risk of addictive illness, emphasizing the importance of diverse treatment modalities and the role of trauma in addiction. The model aims to enhance treatment planning and resource allocation to better address the complexities of addiction recovery.




































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










