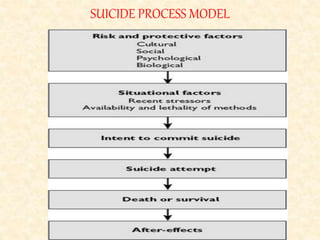
This document discusses suicide risk assessment and prevention. It begins by noting that suicide is a major cause of death worldwide and its epidemiology is changing. It then discusses common myths and facts about suicide, including that suicide attempts should always be taken seriously as an indicator of future risk. Various terminologies related to suicidality are defined, including suicidal ideation, attempts, gestures, and parasuicide. Common risk factors and methods are listed. The document outlines a suicide process model and discusses personality traits like antisocial personality disorder that are associated with suicidality. It concludes by recommending preventive measures like reducing access to lethal means, screening high-risk groups, promoting mental health services, and educating the public