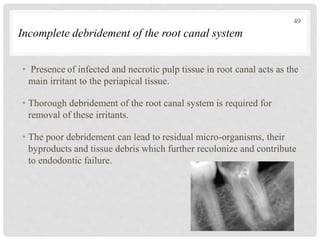
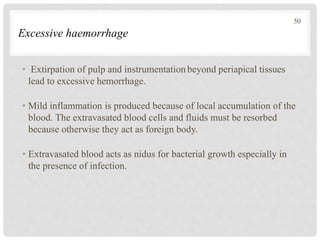
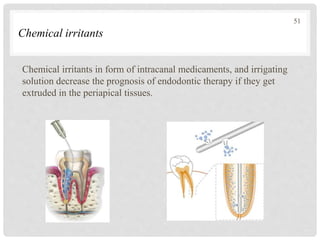
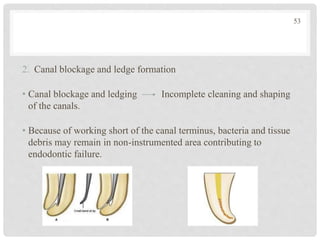
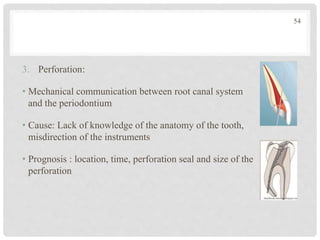
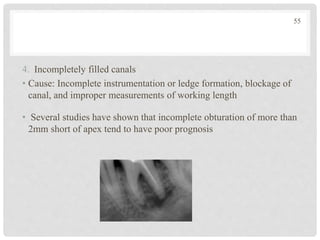
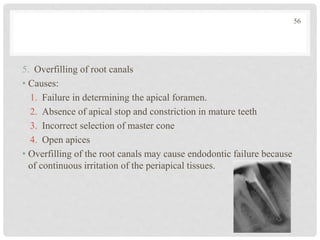
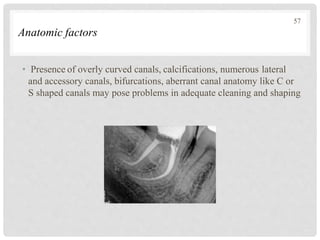
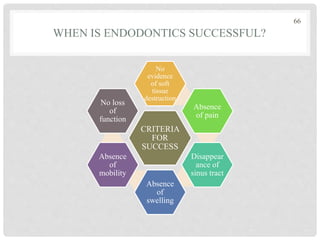
The document discusses the success and failures of endodontics, detailing the definition of treatment success, evaluation criteria, and common factors influencing outcomes. It highlights the success rates of root canal treatments, the impact of various local and systemic factors, and the significance of effective communication with patients regarding treatment prospects. Additionally, it addresses the causes of endodontic failures such as infection, iatrogenic errors, and the role of bacteria like Enterococcus faecalis in persistent infections.