1) Stomach cancer is the third most common cancer worldwide after lung and skin cancer, affecting mostly those aged 50-60. Diet and lifestyle are major risk factors.
2) Risk factors include a diet high in salt, smoked/salted foods, seafood, and carbohydrates but low in vitamins. Chronic conditions like gastritis also increase risk.
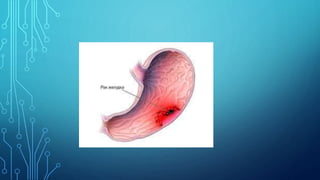
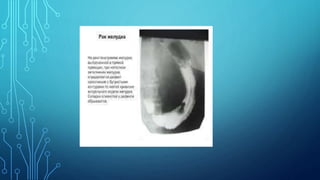
3) Stomach cancer presents with non-specific symptoms like weakness, loss of appetite, weight loss, and epigastric pain or fullness. Diagnosis involves medical history, imaging, endoscopy, and biopsy.
4) Treatment depends on cancer stage and patient health but typically involves surgery to remove part of the stomach, with chemotherapy and





















![Health 10 Ppt[1]. Stomach Cancer](https://cdn.slidesharecdn.com/ss_thumbnails/health10ppt1-stomachcancer-091223081620-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)










![MALIGNANT CANCER OF THE STOMARCH [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/malignantcancerofthestomarchautosaved-250510054659-d24799df-thumbnail.jpg?width=640&height=640&fit=bounds)







































