The document outlines a study that aims to determine if abnormal sensory re-weighting in fall-prone older adults is due to peripheral vestibular loss or central processing deficits, by comparing the postural control and sensory weighting of healthy young adults, healthy older adults, and fall-prone older adults during visual and somatosensory perturbations of varying amplitudes. The study will measure postural sway and gain responses to determine if fall-prone older adults demonstrate heightened sensitivity to visual and somatosensory cues regardless of vestibular function.










![References
1. Allison LK (2006) The dynamics of multi-sensory re-weighting in healthy and
fall-prone older adults. (Doctoral dissertation, University of Maryland, 2006).
Dissertation Abstracts International, 67 (6). (UMI No. 3222601)
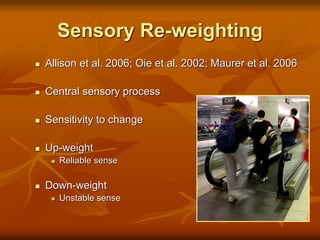
2. Allison LK, Kiemel T, Jeka JJ (2006) Multisensory re-weighting of vision and
touch is intact in healthy and fall-prone older adults. Exp Brain Res 175:342-
352
3. Bertera EM, Bertera RL (2008) Fear of falling and activity avoidance in a
national sample of older adults in the United States. Health Soc Work 33:54-
62
4. Borger LL, Whitney SL, Redfern MS, Furman JM (1999) The influence of
dynamic visual environments on postural sway in the elderly. J Vestibl Res
9:197-205
5. Centers for Disease Control and Prevention [CDC] 2007 Web-based injury
statistics query and reporting system. National Center for Injury Prevention
and Control, Centers for Disease Control and Prevention. Accessed
September 10, 2008 from: www.cdc.gov/ncipc/wisqars
6. Jeka JJ, Allison LK, Saffer M, Zhang Y, Carver S, Kiemel T (2006) Sensory
re-weighting with translational visual stimuli in young and elderly adults: the
role of state-dependent noise. Exp Brain Res 174:517-527
7. Karnath H, Broetz D (2003) Understanding and treating “pusher syndrome.”
Phys Ther 83:1119-1125](https://image.slidesharecdn.com/b0ab5286-d654-4cc9-b3ff-581bf6a53fe3-170213011859/85/SRW-Theory_Methods_Results-12-320.jpg)