Learning Objectives
Tounderstand the indications and contraindications
for basic splinting
To learn the basic equipment necessary for splinting
To understand the technique of splinting
To learn the possible complications of splinting
To provide sources for further information
Indications
Stabilize acuteinjuries, lessen pain and aid healing
Reduces the chance of compartment syndrome
development compared to circumferential casts and
are easier to apply
Casts provide better immobilization and can maintain
reduction of displaced fractures, but higher rates of
complications
5.
Contraindications
No absolutecontraindications
Relative contraindications
Risk of significant increased swelling
Neurovascular compromise
Open fractures – urgent surgical consult required
Significant soft tissue injuries
6.
Equipment
Stockinette
Thinlayer to protect skin
Cut long to extend past edges of split
Soft Roll (Webril Padding)
Layer of soft padding
Select size appropriate for circumference
7.
Equipment
Plaster ofParis
Approximately 10 sheets of rectangular plaster
Requires soaking in room-temperature water
Other materials: scissors, gloves, tape, sheets
Will require preparation: plaster is measured and cut
to appropriate size, soaked in water and wrung
Alternative options:
Pre-fabricated slabs
Fiberglass
8.
Basic technique
Ultimately,the goal of splinting in fracture
management is to immobilize fractures in
acceptable position to aid healing, and to
obtain and maintain an adequate
reduction for displaced fractures
9.
Basic Technique
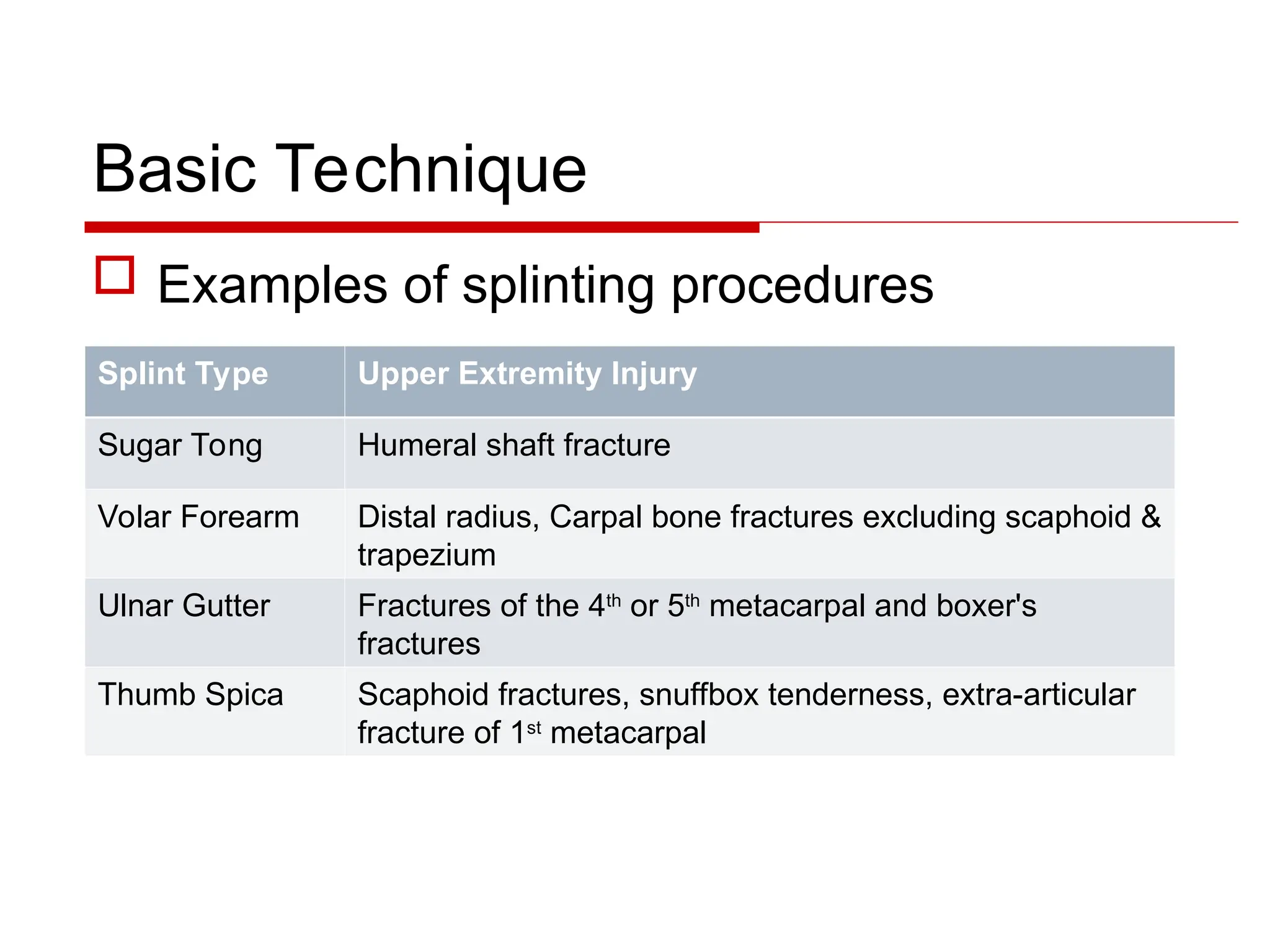
Examplesof splinting procedures
Splint Type Upper Extremity Injury
Sugar Tong Humeral shaft fracture
Volar Forearm Distal radius, Carpal bone fractures excluding scaphoid &
trapezium
Ulnar Gutter Fractures of the 4th
or 5th
metacarpal and boxer's
fractures
Thumb Spica Scaphoid fractures, snuffbox tenderness, extra-articular
fracture of 1st
metacarpal
10.
Basic Technique
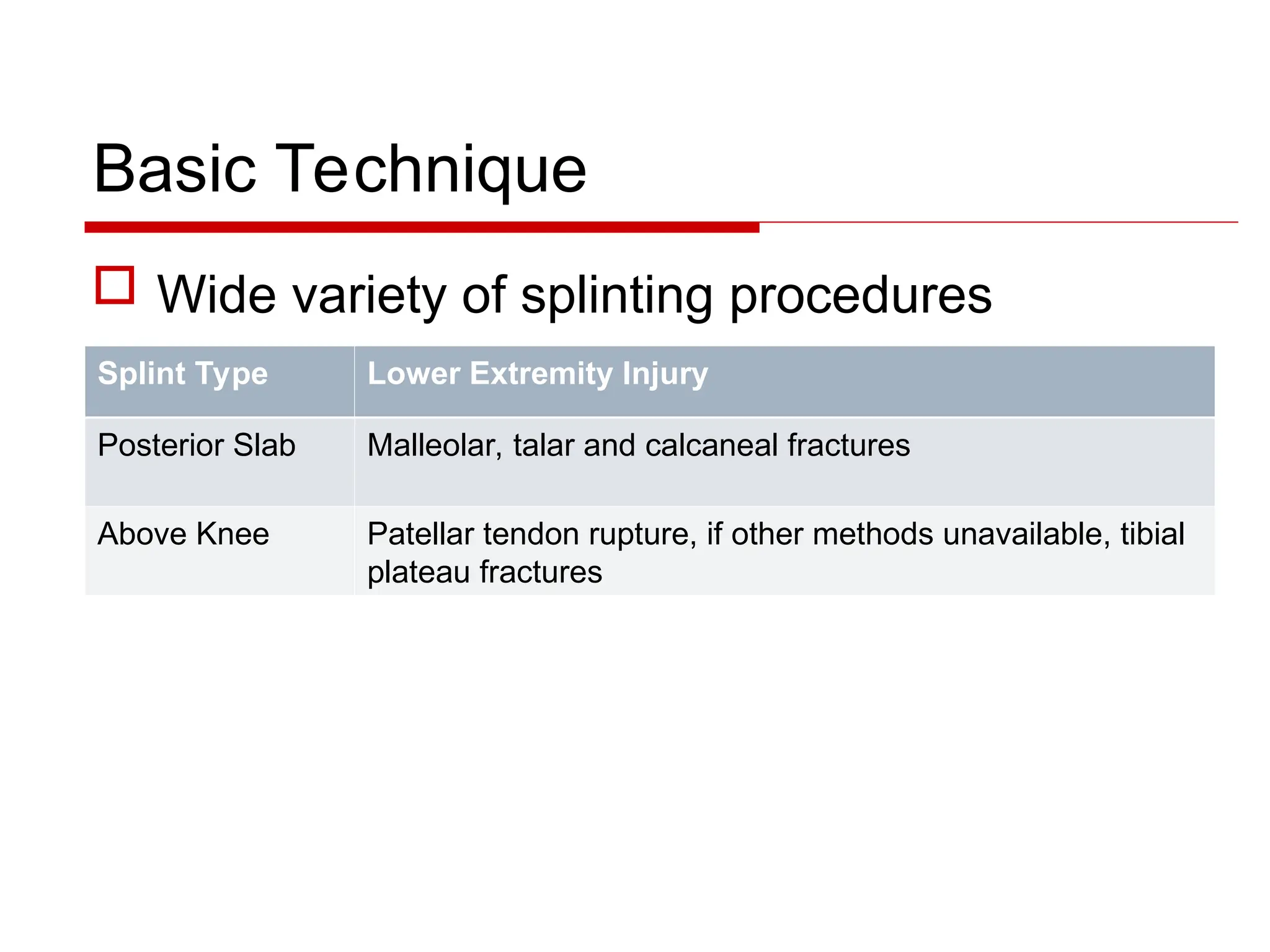
Widevariety of splinting procedures
Splint Type Lower Extremity Injury
Posterior Slab Malleolar, talar and calcaneal fractures
Above Knee Patellar tendon rupture, if other methods unavailable, tibial
plateau fractures
11.
Basic Technique
ATLSprotocol - ensure patient is stable
Expose injured area
Detailed neurovascular exam proximal and
distal to injury, before and after splinting
Consult Orthopaedics for open fractures or
for assistance for splinting where required
(unstable fractures, candidates for operative
management)
12.
Basic Technique
Preparematerials
Select appropriate stockinette size
Cut such that it extends past exposed injured
area
Select appropriate soft roll (outer layer) size
Measure the length of plaster needed
Fill a bucket with room temperature water
13.
Case
A 45year old man is brought into the ER
after slipping at work. He is medically
stable, but is holding his right wrist in pain.
He states he fell forward onto his
outstretched hand. An x-ray reveals a
displaced fracture of his distal radius
(Colles fracture).
15.
Basic Technique: Case1
Colles Fracture: Volar splint
Immobilizes wrist and prevents forearm pronation/supination
Plaster extends from MCP joints to proximal forearm
MCPJs and elbow remain able to flex/extend in cast
Resource: NEJM splinting video
16.
Basic Technique: Volarsplint
Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family
Physician. 2009. 80: 491-499. Figure 7.
Basic Technique: VolarSplint
Set up:
Wrist in supination, 20-30 degrees flexion and
slight ulnar deviation
Apply stockinette
Unroll over arm, well past elbow
Cut a small hole for the thumb
Smooth out, removing wrinkles
20.
Basic Technique: VolarSplint
Apply Soft roll
Unroll from distal to proximal
Just past the elbow, overlapping areas by 50%
Apply extra padding over bony prominences
Apply plaster
Soak 10 sheets of plaster in warm water
Plaster leaves MCPs and elbow free
Smooth out the plaster
21.
Basic Technique: VolarSplint
Molding:
3 point molding to
maintain reduction
Wrist should be in
full pronation, with
slight ulnar
deviation flexion
22.
Case 2
Apatient presents to the ED after an
argument with his girlfriend the previous
evening in which he lost his temper and
punched a wall. He is tender over the
dorsal right 5th
MCP joint and distal
metacarpal. There is no laceration
overlying the dorsal hand. An x-ray is
obtained.
Basic Technique: UlnarGutter
Indication:
Fractures of the 4th
and 5th
metacarpals, “Boxer’s fracture”
Technique:
Wrist is held in slight extension and the 4th
and 5th
MCP joints in
mid-flexion (70-90º),
Stockinette and soft roll extend distally to elbow then folded back
Plaster extends along the ulnar side of the mid-forearm to the 4th
and 5th
DIP joints, with plaster wrapping around these fingers
Additional soft roll & elastic bandage to cover plaster
26.
Basic Technique: UlnarGutter
Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family
Physician. 2009. 80: 491-499. Figure 1.
27.
Basic Technique: ThumbSpica
Indication:
Nondisplaced distal scaphoid fracture (suspected/occult or
visualized on x-ray), extra-articular fracture of 1st
metacarpal
Technique:
The wrist is slightly extended and the thumb in functional
position (“holding a beer can”)
Stockinette and soft roll extend distally to elbow
Plaster extends along the radial aspect of the distal 2/3rds of
forearm to wrapping around the thumb up to the IP joint
Soft roll & elastic bandage to cover plaster
28.
Basic Technique: ThumbSpica
Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family
Physician. 2009. 80: 491-499. Figure 2.
29.
Basic Technique: PosteriorAnkle Splint
Indication:
Malleolar, talar, calcaneal fractures and Achilles tendon tears
Technique:
Patient prone, ankle is in 90º flexion
For Achilles tear, ankle is immobilized in plantar flexion
Stockinette and soft roll extend just distal to knee
Plaster extends from the MTPs along the plantar aspect of
the foot, ankle and posterior calf ending 2 inches distal to the
posterior knee
30.
Basic Technique: PosteriorAnkle Splint
Boyd A, Benjamin H and Asplund. C. Splints and
Casts: Indications and Methods. American Family
Physician. 2009. 80: 491-499. Online Figure G.
Note: Ankle fractures should be
treated with a three sided splint
(ie: Posterior Ankle + Stirrup)
31.
Basic Technique: StirrupSplint
Indication:
Malleolar, talar and calcaneal fractures
Technique:
The ankle is in 90º flexion
Stockinette and soft roll extend just distal to knee
Plaster extends from the lateral aspect of the mid-calf around
the heel to the medial aspect of the mid-calf.
Similar to sugar-tong splint
Additional soft roll and elastic bandage for stabilization
32.
Basic Technique: StirrupSplint
Boyd A, Benjamin H and Asplund. C.
Splints and Casts: Indications and
Methods. American Family Physician.
2009. 80: 491-499. Online Figure H.
Note: Ankle fractures
should be treated with
a three sided splint
(ie: Posterior Ankle +
Stirrup)
33.
Trouble-shooting
Water shouldbe warm
Too cold – requires a longer set time
Too hot – increased risk of thermal injuries
Smooth out wrinkles or creases in plaster to
reduce risk of pressure sores
Ensure adequate soft roll coverage over bony
prominences
Distal neurovascular exam before and after
casting
34.
Complications
Thermal injuries:Plaster setting is an exothermic reaction,
ensure the water used to soak the plaster is warm
Pressure sores: Caused by uneven plaster, wrinkles or
creases. Ensure adequate soft roll over bony prominences
and smooth out the plaster as it sets
Compartment syndrome, less likely with splints than casts
To avoid, ensure injured area has enough room to swell
If compartment syndrome occurs, immediately remove splint
Assess limb for ischemic injury
Lack of stability and re-injury from poor immobilization
35.
Case 1, revisited
Your patient has a volar splint applied for
their Colle’s fracture. However, he returns
several days later complaining of pain and
irritation in the area of his ulnar styloid.
Upon inspection you find a depression in
the plaster material and the bony
prominence is only covered by one layer of
soft roll.
36.
Case 1, revisited
Resolution: Pressure sores by result from creases or
folds in plaster material or inadequate soft roll
coverage, often over bony prominences
Ensure several layers of soft roll cover areas of bony
prominence
Ensure the plaster is smoothed out and immobilized
until it is fully set to avoid creases
37.
Links to ProceduralVideos
NEJM splinting video:
http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Ulnar gutter splint:
http://www.youtube.com/watch?v=kx2YBmq7oS0
Thumb spica splint:
http://www.youtube.com/watch?v=864h9gVgmKs
38.
Quiz Question 1
When compared to casts, splints:
A. Better reduce immobilization injuries
B. Provide superior stability
C. Reduce compartment syndrome
D. More difficult to apply
39.
Quiz Question 2
A patient in the ED has an open fracture of his fibula. You
should:
A. Splint the fracture to prevent compartment syndrome
B. Apply a circumferential leg cast
C. Consult orthopaedic surgery
D. Apply a tensor bandage
40.
Quiz Question 3
For a displaced fracture of the distal radius,
the most appropriate splint to apply is:
A. Sugar tong splint
B. Volar slab
C. Radial gutter splint
D. Short arm cast
41.
Quiz Question 4
You assess a patient in the ED who has recently
punched a wall during a fight. X-rays show a fracture
of the distal fifth metacarpal, also known as a Boxer’s
fracture. The most appropriate splint to apply is:
A. Volar forearm splint
B. Radial gutter splint
C. Thumb spica splint
D. Ulnar gutter splint
42.
Quiz Question 5
Good splinting technique does not include which of
the following:
A. The plaster is soaked in hot water
B. Stockinette that extends past the area to be splinted
C. Soft roll coverage, especially over bony prominences
D. Wrinkles and creases are smoothed out as the plaster
sets
43.
Summary
Splinting iseffective for acute management of bony
injuries (fractures) and some soft tissue injuries
The primary advantage of splinting over
circumferential casts is that they allow for acute
swelling and are easier to apply
Consult Orthopedics for open fractures or those in
which reduction is not adequately obtained or not
anticipated to be maintained (unstable fractures), or
fractures involving neurovascular compromise
44.
General References
JournalArticles:
Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family
Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008.
http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Chapters in Textbooks:
Simon, R and Sherman S. Emergency Orthopedics, 6th
ed. 2011. McGraw-Hill.
AO foundation:
https://www.aofoundation.org
Wheeless Online: Textbook of Orthopaedics
http://www.wheelessonline.com/
Web Links
http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Editor's Notes
#4 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499.
#9 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499.
#10 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
#11 Supplementary Information
(Please refer to “Supplementary Information” document for instructions)
Notes:
Instructions:
Answers to questions:
Specific References: Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
#12 Supplementary Information
(Please refer to “Supplementary Information” document for instructions)
Notes:
Instructions:
Answers to questions:
Specific References: Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
#14 Personal photo provided by Dr. Nazanin Meshkat, 2015.
#15 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Jupiter, J. AO Foundation, “Distal radius fractures” 23-A2.3. https://www2.aofoundation.org/
#16 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499. Online Figure H.
#17 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499. Online Figure H.
#19 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
#20 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
#21 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Jupiter, J. AO Foundation, “Distal radius fractures” 23-A2.3. https://www2.aofoundation.org/
#23 Ask learners to identify the fracture on both images. (Right D5 metacarpal head fracture; Boxer’s fracture)
Personal photo provided by Dr. Nazanin Meshkat, 2015.
#24 Ask learners to identify the fracture on both images.
Personal photo provided by Dr. Nazanin Meshkat, 2015.
#25 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Simon, R and Sherman S. Emergency Orthopedics, 6th ed. 2011. McGraw-Hill.
#26 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499. Online Figure H.
#27 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Simon, R and Sherman S. Emergency Orthopedics, 6th ed. 2011. McGraw-Hill.
#28 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499. Online Figure H.
#29 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Simon, R and Sherman S. Emergency Orthopedics, 6th ed. 2011. McGraw-Hill.
Position of plantar flexion that the patient is splinted in should be in ‘gravity equinus’, meaning the degree of plantar flexion that the free hanging foot is in when the patient is seated on the edge of a stretcher with their foot dangling in the air.
#30 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499. Online Figure H.
#31 Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
Fitch, M et al. Videos in Clinical Medicine: Basic Splinting Techniques. NEJM. 2008. http://www.nejm.org/doi/full/10.1056/NEJMvcm0801942
Simon, R and Sherman S. Emergency Orthopedics, 6th ed. 2011. McGraw-Hill.
#32 Boyd A, Benjamin H and Asplund. C. Splints and Casts: Indications and Methods. American Family Physician. 2009. 80: 491-499. Online Figure H.
#34 Specific References: Boyd A, Benjamin H and Asplund. C Spints and Casts: Indications and Methods. Amierican Family Physician. 2009. 80: 491-499.
#39 Correct Answer: C
Depending on the nature of the injury (how open it is, how badly displaced, how much swelling, etc), it is often advisable to splint the fracture temporarily to reduce and immobilize the injury prior to being taken to the OR, depending on when your orthopedics colleagues are planning to operate. This is in addition to updating tetanus status, giving IV antibiotics, gently cleaning the wound and applying sterile gauze to the wound site. So in many cases you will also do “A” as well as “C”, albeit in consultation with your colleagues in orthopedics.