Recommended

More Related Content
What's hot
What's hot (18)
Similar to SocietyofBehaviorMedicine2015
Similar to SocietyofBehaviorMedicine2015 (20)
SocietyofBehaviorMedicine2015
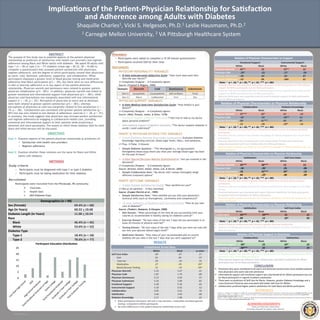
- 1. RESEARCH POSTER PRESENTATION DESIGN © 2012 www.PosterPresentations.com The purpose of this study was to examine aspects of the patient-physician relationship as predictors of satisfaction with health care providers and regimen adherence among Black and White adults with diabetes. We asked 99 adults with type 1 (n = 18) or type 2 (n = 77) diabetes (mean age = 60.32, SD = 10.68) to complete a questionnaire that assessed patient satisfaction with physicians, regimen adherence, and the degree to which participants viewed their physicians as warm, cold, dominant, submissive, supportive, and collaborative. White participants displayed a greater level of blood glucose testing and medication adherence than Black participants (p’s < .05), but there were no race differences in diet or exercise adherence or in any aspect of the patient-physician relationship. Physician warmth and dominance were related to greater patient- physician collaboration (p’s< .001). In addition, physician warmth was linked to greater emotional and informational support from physicians (p’s < .001), while physician cold-heartedness was marginally associated with less informational support (r = -.18, p = .07). Perception of physicians as warm and as dominant were both related to greater patient satisfaction (p’s < .001), whereas perceptions of physicians as cold was marginally related to less satisfaction (r = -. 19, p = .06). Collaboration was correlated with greater patient satisfaction (p < . 001) but was only related to one domain of adherence: exercise (r = .26, p = .01). In summary, this study suggests that physicians may increase patient satisfaction and regimen adherence by engaging in collaborative health care, providing emotional and informational support to their patients while projecting a dominant and warm personality. The extent to which these relations held for both black and white persons will be discussed. ABSTRACT Goal 1: Examine aspects of the patient-physician relationship as predictors of: • Satisfaction with health care providers • Regimen adherence Goal 2: Examine whether these relations are the same for Black and White adults with diabetes OBJECTIVES CONCLUSION ACKNOWLEDGEMENTS Shaquille Charles1, Vicki S. Helgeson, Ph.D.1 Leslie Hausmann, Ph.D.2 1 Carnegie Mellon University, 2 VA PiNsburgh Healthcare System ImplicaDons of the PaDent-‐Physician RelaDonship for SaDsfacDon and Adherence among Adults with Diabetes METHODS Study criteria – Participants must be diagnosed with type-1 or type-2 diabetes – Participants must be taking medication for their diabetes Recruitment Participants were recruited from the Pittsburgh, PA community Ø Churches Ø Health fairs Ø ADA Diabetes Expo Procedure • Participants were asked to complete a 15-20 minute questionnaire • Participants received $20 for their time Instruments PHYSICIAN PERSONALITY VARIABLES Ø 8-item Interpersonal Adjective Scale: “How much does each item describe your doctor?” (1=Completely Disagree — 6=Completely Agree) Source: (Trapnell & Wiggins, 1990) PHYSICIAN SUPPORT VARIABLES Ø 6-item Medical Interview Satisfaction Scale: “How helpful is your doctor?” (1=Completely Disagree — 6=Completely Agree) Source: (Wolf, Putnam, James, & Stiles, 1978) • Emotional Support (Affective Subscale): “I feel free to talk to my doctor about personal problems” • Informational Support (Cognitive Subscale): “The doctor explains diabetes in words I could understand” PAIENT & PHYSICIAN INTERACTIVE VARIABLES Ø 5-item Diabetes-Related Knowledge Assessment: Evaluates diabetes knowledge regarding exercise, blood sugar levels, HbA1c, and symptoms. (1=True, 2=False, 3=Unsure) • Sample Diabetes Question : “The Hemoglobin A1C (or glycosylated hemoglobin) blood assay shows you what your average blood sugar has been for the past 24 hours” Ø 3-item Shared Decision-Making Questionnaire: “Are you involved in the decisions?” (1=Completely Disagree — 6=Completely Agree) Source: (Kriston, Scholl, Holzel, Simon, Loh, & Harter, 2009) • Sample Collaboration Item: “My doctor and I always thoroughly weigh different treatment options” PAIENT OUTCOME VARIABLES Ø 4-item Patient Satisfaction Scale: “How satisfied are you?” (1=Not at all satisfied — 4=Very Satisfied) Source: (Cooper-Patrick et al., 1999) • Sample Satisfaction Item: “How satisfied are you with your physician’s technical skills (such as thoroughness, carefulness and competence)?” Ø 12-item Summary of Diabetes Self-Care Activities: “How do you take care of diabetes?” Source: (Toobert, Hampson, & Glasgow, 2000) • Diet Domain: “What percentage of the time do you successfully limit your calories as recommended in healthy eating for diabetes control?” • Exercise Domain: “On how many of the last 7 days did you participate in at lease 20 minutes of physical exercise?” • Testing Domain: “On how many of the last 7 days (that you were not sick) did you text your glucose (blood sugar) level?” • Medication Domain: “How many of your recommended pills to control diabetes did you take in the last 7 days that you were supposed to?” Thank you Tiona Jones, Gianna Davis and Katilyn Mascatelli for aiding in data collection Domain: Warmth Cold Dominance Submissive Item 1: Sympathe/c Unsympathe/c Self-‐confident Timid Item 2: Warm Coldhearted Firm Shy RESULTS RelaDon of Physician CharacterisDcs to Support EmoDonal Support Instrumental Support White Black White Black Physician Warmth .43** .18 .42** .22 Physician Cold -‐.28* -‐.02 -‐.27+ -‐.06 Physician Dominance -‐.04 .26+ -‐.05 .07 Physician Submissive -‐.07 .09 -‐.004 .01 Note: + p < .10; * p < .05; ** p < .01, *** p < .001 RelaDon of Physician CharacterisDcs to Physician RelaDonship CollaboraDon Diabetes Knowledge White Black White Black Physician Warmth .47*** .35* .14 -‐.14 Physician Cold -‐.02 -‐.10 -‐.36** .15 Physician Dominance .25+ .51*** .10 .07 Physician Submissive .12 -‐.20 -‐.29* -‐.15 Note: + p < .10; * p < .05; ** p < .01, *** p < .001 § Physician Warmth associated with more Collabora/ve Health Care for both Black and White par/cipants. § Physician Cold was related to less Diabetes Knowledge for White par/cipants but not for Black par/cipants. § Physician Dominance was correlated with more Collabora/on for Black par/cipants but marginally associated with more Collabora/on for White par/cipants. § Physician Submissiveness was linked to less Diabetes Knowledge for White par/cipants but not Black Par/cipants. RelaDon of Physician CharacterisDcs to Physician RelaDonship SaDsfacDon Self-‐Care Index White Black White Black Physician Warmth .59*** .58*** .12 .12 Physician Cold -‐.10 -‐.26+ -‐.01 -‐.06 Physician Dominance .18 .52*** .33* -‐.12 Physician Submissive .04 -‐.29+ -‐.06 -‐.09 Note: + p < .10; * p < .05; ** p < .01, *** p < .001 Comparisons Across Race White Black p-‐value Self-‐Care Index .09 -‐.07 .17 Diet .01 .00 .97 Exercise .09 -‐.10 .32 Medica/on .27 -‐.05 .05* Blood Glucose Tes/ng .21 -‐.19 .04* Physician Warmth 5.33 5.47 .41 Physician Cold 1.87 1.79 .80 Physician Dominance 5.13 5.03 .57 Physician Submissive 2.16 2.09 .81 EmoDonal Support 5.28 5.39 .65 Instrumental Support 5.10 5.42 .12 CollaboraDon 4.95 5.01 .76 SaDsfacDon 3.46 3.50 .68 Diabetes Knowledge 2.17 1.98 .43 § Black par/cipants had poorer self-‐care in two domains—medica/on and blood glucose tes/ng—compared to White par/cipants § No other differences in the pa/ent-‐physician rela/onship across race § Physician Warmth was related to greater Physician Sa/sfac/on for both White and Black par/cipants. § Physician Cold was marginally linked to less Pa/ent Sa/sfac/on for Black people but not White people. § Physician Dominance was associated with higher Physician Sa/sfac/on for Black par/cipants but greater Self-‐Care behaviors for White par/cipants. § Physician Submissiveness was linked to less Physician Sa/sfac/on for Black par/cipants but not White Par/cipants. RelaDon of Physician CharacterisDcs to Physician RelaDonship SaDsfacDon Self-‐Care Index White Black White Black CollaboraDon .53*** .59*** .15 .21 Diabetes Knowledge .09 .13 .33* .05 Note: + p < .10; * p < .05; ** p < .01, *** p < .001 § Pa/ent-‐Physician Collabora/on was related to greater Physician Sa/sfac/on § Diabetes Knowledge was linked to the beNer Self-‐Care behavior for White par/cipants but not Black par/cipants RelaDon of Physician Support to Outcomes CollaboraDon SaDsfacDon White Black White Black EmoDonal Support .30* .23 .32* .22 InformaDonal Support .50*** .22 .39** .22 Note: + p < .10; * p < .05; ** p < .01, *** p < .001 § Emo/onal Support was correlated with more Collabora/on and Physician Sa/sfac/on for White par/cipants but not for Black par/cipants. § Informa/onal Support was linked to more Collabora/on and Pa/ent Sa/sfac/on for White par/cipants but not for Black par/cipants. § Physician Warmth was associated with greater physician Emo/onal Support and Informa/onal Support for White par/cipants but not Black par/cipants. § Physician Cold was correlated with less Emo/onal Support and a marginally less Informa/onal Support for White par/cipants but not Black par/cipants. § Physician Dominance was marginally linked to more Emo/onal Support for Black par/cipants but not White par/cipants. § Physicians who were considered to be warm and dominant tend to have more sa/sfied pa/ents than physicians who were cold and submissive § Informa/onal support and emo/onal support was only beneficial for White par/cipants but not for Black par/cipants in regards to pa/ent sa/sfac/on § There were no predictors of Self-‐Care for Blacks. However, greater Diabetes Knowledge and a more Dominant Physician was associated with beNer Self-‐Care for Whites § Collabora/on predicted higher pa/ent sa/sfac/on for both Black and White par/cipants Demographics (n = 99) Sex (Female) 69.4% (n = 68) Age (In Years) 60.32 + 10.68 Diabetes Length (In Years) 11.00 + 10.54 Race Black 46.4% (n = 45) White 53.6% (n = 52) Diabetes Type Type-‐1 18.4% (n = 18) Type-‐2 78.6% (n = 77) 0 5 10 15 20 25 ParDcipant EducaDon DistribuDon REFERENCES • Toobert, D. J., Hampson, S. E., Glasgow, R. E. (2000). The summary of diabetes self-‐care ac/vi/es measure: Results from 7 studies and a revised scale. Diabetes Care, 23(7), 943-‐950. • Cooper-‐Patrick, L., Gallo, J. J., Gonzales, J. J., Vu, H. T., Powe, N. R., Nelson, C., et al. (1999). Race, gender, and partnership in the pa/ent-‐physician rela/onship. Journal of the American Medical AssociaDon, 282(6), 583-‐589. • Kriston, L., Scholl, I., Hölzel, L., Simon, D., Loh, A., & Härter, M. (2010). The 9-‐item Shared Decision Making Ques/onnaire (SDM-‐Q-‐9). Development and psychometric proper/es in a primary care sample. PaDent EducaDon and Counseling, 80(1), 94-‐99.