Case Presentation
A 14Years old male patient had ON and OFF complaints of of
Shortness of breath which progressed gradually , Cough with
expectoration , Loss of appetite and associated weight loss – 4kg since
november 2024 . no history of any comorbities . NO significant past
history
• Birth History –
Term baby, mode of delivery – LSCS
Birth weight - 4.5kg
Non consanguineous marriage
CECT CHEST doneoutside on 13/02/25
• Patchy consolidatory changes with air bronchogram
seen in anterior segment of right upper lobe
• Multiple enlarged by perihilar, paratracheal and
mediastinal lymph nodes seen compressing the
adjacent structures
• Patient was started on empirical ATT therapy.
5.
• Bronchoscopy (outisidecenter) done on 22/2/25 showed
right main bronchus obliterated with extensive compression
• Right middle lobe bronchus was not seen, right lower lobe
bronchus necrotic debris was seen
• BAL analysis was done which showed
GeneXpert -MTB - Negative
AFB smear- Negative
FUNGAL KOH mount -negative
• Following this EBUS was done on 25/2/25 which showed
Negative for granulomas and malignancy
7.
SYMPTOMS DOESNT RESOLVE- PET-CT done
• Showed Right supraclavicular lymph
node 1.3* 0.7cm (SUV max 4.91)
• FDG avid discrete and conglomerated
upper and lower paratracheal,
• perivascular, subcarinal and right
hilar
• LN (5.9x5.6x5.4cm) SUV 25.88. Lesion
• encases right pulmonary artery and
right main bronchus.
• Moderate pericardial effusion seen.
• Hepatomegaly
• FNAC - Supraclavicular LN (17/3/25)
showed Reactive hyperplasia.
8.
2D echo showedlarge pericardial effusion with ejection fraction 60%,
normal biventricular function, trivial MR/TR/mild PAH.
Pericardiocentesis was done.
Pericardial fluid analysis -
ADA 9.8 (normal=0 t0 30), LDH for 25, protein 6.27, glucose 97, albumin
2.51.
MTB not detected.
Cytology revealed - lymphocytic effusion with few eosinophils
9.
Then, Referred toour centre
• On clinical examination patient had severe SOB
• Cough with thin mucoid expectoration
• LAB PARAMETERS Normocytic normochromic,
leukocytosis with eosinophilia.
• LFT , serum creatinine - normal limits.
• .
CECT CHEST
Bilateral mildpleural effusion with subsegmental collapse of underlying lung.
Patchy areas of consolidation with adjacent minimal ground glassing noted in anterior segment of
left
upper lobe, left lingula, posterior segment of right upper lobe, lateral segment of right middle lobe
and
also in basal segments of both lower lobes. Post-contrast no obvious enhancement detected.
===> Possibly infective aetiology
12.
Ill-defined soft tissue
densitynoted in
mediastinum completely
encasing the mediastinal
vessels, mediastinal lymph
nodes with lateral extension
into adjacent hila causing
mild to moderate
compression pulmonary
vessels, superior and
inferior vena cava with
associated minimal to mild
compression bilateral Atria
noted.
Post-contrast there is mildly
enhancing noted.
There is thin irregular
peripheral calcific specks
involving pericardium in
superior mediastinum
noted.
Few prominent enhancing
prevascular, right and left
paratracheal lymph nodes
noted within the above
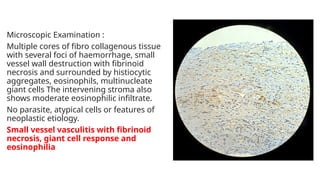
Microscopic Examination :
Multiplecores of fibro collagenous tissue
with several foci of haemorrhage, small
vessel wall destruction with fibrinoid
necrosis and surrounded by histiocytic
aggregates, eosinophils, multinucleate
giant cells The intervening stroma also
shows moderate eosinophilic infiltrate.
No parasite, atypical cells or features of
neoplastic etiology.
Small vessel vasculitis with fibrinoid
necrosis, giant cell response and
eosinophilia
17.
FURTHER WORKUP
C-ANCA/P-ANCA –Negative
ANA By IF – Negative
Fungal Workup – Negative
Parasitic workup – Negative
Serum IgG4 – 11.60 g/L (0.03 – 2.0)
Total Serum IgG – 2245.18 mg/dL
Sr. IgG4/Sr. IgG – 51.7%
Treatment Received -
•3 Doses of Pulse corticosteroids – Inj. Methyl Prednisolone 10mg/kg
• Followed by Inj Methyl Prednisolone1mg/kg.
• Patient Recovered well with weaned off oxygen support within
3 days of treatment.
20.
followup scan duringtreatment CT 05/ 04/2024
As compared to previous CT dated 28th March 2025 :
There is significant decrease in bilateral pleural effusion.
There is complete resolution of passive collapse of posterobasal segment of right lower
lobe