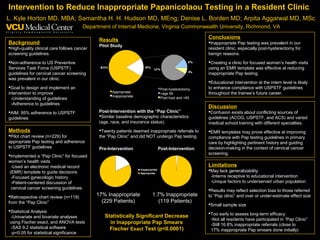
The study found that 17% of Pap tests ordered in their resident clinic were inappropriate based on USPSTF guidelines. They created an intervention called the "Pap Clinic" which used an EMR template to guide decision making and patient discussions about cervical cancer screening guidelines. After implementing this clinic, they found a statistically significant decrease in inappropriate Pap tests, from 17% pre-intervention to 1.7% post-intervention. While the results were promising, the study had limitations including a small sample size and potential for selection bias. The intervention showed that templates in EMRs have potential to improve adherence to screening guidelines.