Includes:
1. Acute generalizedexanthematous pustulosis
2. Drug reaction with eosinophilia and systemic symptoms(DRESS)
3. Drug induced generalized exfoliative dermatitis
‐
4. Stevens–Johnson syndrome/toxic epidermal necrolysis
3.
Acute generalized exanthematous
pustulosis(Exanthemic pustular psoriasis /Toxic
pustuloderma /Pustular drug rash)
Incidence:1–5 per million per year
mean age of onset :56 years
male to female incidence ratio of 0.8
Associated diseases: infections such as Mycoplasma pneumoniae, coxsackievirus [8], parvovirus B19 and
cytomegalovirus (CMV) .
Mercury exposure and spider bites have also been associated
Pathophysiology:
1. Drug specific CD4+ and CD8+ cells are involved
‐
2. high level of CXCL8 ( a proinflammatory cytokine) production.
3. subtypes of T cells producing interleukin (IL) 8, a neutrophil attracting chemokine
‐ have also been
identified in the peripheral blood of patients with AGEP.These are important in the pathogenesis of the
sterile pustules seen in this disease process, by attracting neutrophils into the already oedematous skin and
creating pustules.
4. mutations in the IL36RN gene, which codes for the IL 36 receptor antagonist (IL 36Ra) are also involved
‐ ‐
4.
Predisposing factors:
most commonlyassociated agents :
• Pristinamycin
• Aminopenicillins
• Quinolones
• chloroquine
• hydroxychloroquine,
• Sulphonamides
• terbinafine
• diltiazem
Less commonly associated drugs :
• corticosteroids
• other macrolide antibiotics,
• non steroidal anti inflammatory
‐ ‐
drugs of the oxicam class
• antiepileptic medications (except
valproate)
5.
Histopathology :
1.is characterized by marked spongiosis affecting the dermis
and epidermis, accompanied by intraepidermal pustules
and vesicles along with marked to moderate papillary
dermal oedema
2. A perivascular infiltrate occurs, which is usually
neutrophilic. Occasional eosinophils may be seen but are
not invariably present.
3. There are infrequent necrotic keratinocytes .
4. The classic histopathological features of psoriasis are
absent, which is important in distinguishing the presentation
of AGEP from its closest differential, pustular psoriasis.
6.
Clinical features
Exposureto the culprit drug typically occurs between 2- 5 days
prior to the onset of the eruption. This short latency is typical
of AGEP.
A prodrome of burning or itching in the skin may occur and the
patient may be asthenic.
Sheets of hundreds of sterile non follicular pustules are seen
‐
arising most commonly in the major flexures such as the neck,
axillae and inframammary and inguinal folds. However, non flexural
‐
sites may be involved.
The pustules typically arise on a background of oedematous
erythema.
Less commonly described clinical features include atypical targets,
purpura, blisters and vesicles.
Mucous membrane involvement is rare, and if present, is mild and
generally limited to one site, usually the mouth.
Systemically, the patient may be febrile. A leucocytosis, typically a
neutrophilia may be present. Eosinophils are less commonly
elevated
7.
A setof diagnostic criteria was proposed by Roujeau et al. as
follows:
1. Appearance of hundreds of sterile non follicular pustules at
‐
flexural sites.
2. Histopathological changes of spongiosis and epidermal
pustule formation.
3. Fever >38°C.
4. Blood neutrophil count >7 × 109/L.
5. Acute evolution
AGEP is generally rapid in both onset and resolution
Clinical variants:
A localized form of AGEP, called acute localized exanthematous
pustulosis (ALEP), is characterized by pustules confined to a single
body area, most commonly the neck. A similar clinical course of
short latency, rapid recovery and lack of recurrence is seen
8.
AGEP Pustular Psoriasis
Historyof psoriasis Possible Common
Distribution pattern Predominance in the folds More generalized
Duration of pustules Shorter Longer
Duration of fever Shorter Longer
History of drug reaction Usual Uncommon
Recent drug administration Very frequent Less frequent
Arthritis Rare ∼30%
Histology Spongiform subcorneal and/
or intraepidermal pustules,
oedema of papillary dermis,
vasculitis, exocytosis of
eosinophils, single cell
‐
necrosis of keratinocytes
Subcorneal and/or
intraepidermal pustules,
papillomatosis, acanthosis
9.
Differential diagnosis
Pustular psoriasis
(theVon Zumbusch variant)
Subcorneal pustular dermatosis (Sneddon–Wilkinson
disease) :may be distinguished by its less acute
course, and the presence of flaccid pustules which
demonstrate a hypopyon sign
DRESS :pustules will generally be less
numerous in than in AGEP ,also invariably
have systemic involvement of an internal
organ, while this is less common in AGEP.
Candida infection :can present with
pustules in flexural sites (but can be
distinguished by clinical context and
detection on microbiological
testing)
10.
Complications andco morbidities
‐ :The patient must avoid the culprit drug
and related compounds following the episode. No other sequelae are
described.
Disease course and prognosis :The prognosis in AGEP is excellent and full
recovery is to be expected.
Investigations :In most cases a careful drug history is adequate to elucidate
the culprit drug
1. A skin biopsy should be taken early in the disease presentation as it will assist
in the distinction from pustular psoriasis.
2. Baseline haematological investigations, looking for neutrophilia and
eosinophilia
3. Biochemical investigations should be performed to rule out renal and liver
dysfunction, as well as hypocalcaemia.
4. Biochemical of acute phase reactants such as C reactive protein (CRP)
‐ may
help to distinguish infection from the systemic involvement in AGEP. A septic
screen may be done if suspicion of infection is high.
11.
Management :
1.Corticosteroid therapy:
• If the patient appears systemically well, with limited areas of
involvement, potent topical corticosteroid may suffice.
• In cases of more extensive involvement, or where systemic features such as
fever, haemodynamic compromise or systemic upset are seen, oral
corticosteroids may be required. (Intravenous administration is not usually
necessary)
2. Emollient therapy : should be prescribed, and continued throughout the
phase of postpustular desquamation, until full skin integrity is restored.
3. In cases where systemic involvement such as renal impairment or liver
function disturbance is noted, appropriate supportive care such as
intravenous fluids and careful haemodynamic monitoring should be done
4. If the patient is febrile, care should be taken to exclude an infective
source, and if suspicion of this remains, then empiric antibiotic therapy
should be considered.
12.
DRESS isan idiosyncratic multisystem drug hypersensitivity disorder.
It is characterized by cutaneous rash, which may be of variable morphology, and systemic
involvement along with fever and lymphadenopathy
Incidence of DRESS : 1 in 1000 to 1 in 10 000
mean age of onset : 48 years
Has a a slight female preponderance, with a male to female ratio of 0.8
Drug reaction with eosinophilia and
systemic symptoms
1. Drug specificT cell theory
‐ ‐ 2. Viral reactivation theory
Haptenization theory The p i concept
‐
• Haptenization : the process whereby a small
immunologically neutral molecule is rendered
antigenic when bound to a protein
• In order for this binding process to occur, the drug
must first undergo enzymatic degradation
• one possible locus of susceptibility to DRESS might
be polymorphisms in the genes that encode these
enzymes
• ‘pharmacological interaction
of drugs with the immune
receptor’
• A drug molecule may bind directly to the
major histocompatibility complex (MHC) via
a protein bound to the MHC, or may insert
itself in to the MHC groove(without
undergoing haptenization)
• The part of the antigen presenting cell (APC) presented to the
‐
T cell receptor will be reconfigured, thus provoking a T cell response. If
‐ ‐
the drug modified structure is subsequently recognized by a T cell in
‐
the context of costimulation, then a cascade effect of the T cell
‐
response occurs.
Pathophysiology: The two main theories are that of a drug specific T cell reaction,
‐ ‐
and that of viral reactivation
based on the principle that a given drug may elicit a
T cell reaction specific to that medication.
‐
15.
2. Viral reactivationtheory :
Herpesvirus reactivation has been demonstrated to occur in DRESS :The
implicated viruses have included HHV 6, CMV, Epstein–Barr Virus (EBV) and
‐
HHV 7
‐
Virus reactivation appears to occur in a sequential fashion, with HHV 6 and
‐
EBV being detected earlier in the course of the disease, followed by HHV 7
‐
and CMV
It has been postulated that a drug induced immunosuppressed state,
‐
characterized by hypogammaglobulinaemia, facilitates the initial
reactivation of latent herpesvirus
The sequential nature of viral reactivation suggests a correlation with the
clinical phases of DRESS. Rash and fever are often the first presenting
features, followed by lymphadenopathy and internal organ dysfunction
there is a complex interplay between virus, the host immune response to
the virus and a drug specific immune response, which produces the clinical
‐
picture
16.
Histopathology :
1.Common features seen include spongiosis, a superficial
perivascular lymphocytic infiltrate and an eosinophilic infiltrate
in the dermis
2. Other findings: A lichenoid infiltrate may be seen .
3. In some cases, basal cell vacuolar change, with the
presence of necrotic keratinocytes has been noted, with
changes resembling erythema multiforme (EM)
4. presence of EM like changes histopathologically and more
‐
severe liver dysfunction may be predictive of a higher
mortality
17.
GENETICS:
HYPERSENSITIVITY TO DRUG:HLA association
Abacavir HLA B*5701
‐
Carbamazepine HLA B*1502
‐ and HLA B*3101, HLA DR3
‐ ‐
and HLA DQ2
‐
Allopurinol HLA B*5801
‐
Lamotrigine HLA-B*1502
Phenytoin HLA-B*1502
18.
CLINICAL FEATURES
History:
Patientstypically describe a prodromal phase characterized by asthenia, malaise
and fatigue. They may have a fever.
The appearance of a rash, accompanied by facial swelling, is usually the first
clinical feature to emerge, and may provoke the patient to seek medical
attention.
The drug history should be elicited carefully in such patients, as a considerable
period of time, between 2 and 6 weeks, may have elapsed between ingestion of
the culprit drug and the onset of symptoms.
Presentation:
DRESS is characterized by a rash suspected to be drug induced, accompanied by
a fever, lymphadenopathy and systemic upset, the latter referring to derangement
of the function of at least one organ system, and haematological abnormalities
19.
The most commonvariant - the urticated
papular exanthem which consists of
widespread papules and plaques, often
accompanied by cutaneous oedema
A morbilliform eruption
Erythroderma characterized by a
widespread exfoliative erythema
erythema multiforme like features in
‐
the skin, developing dusky or purpuric
atypical targets
20.
An importantclinical finding in the majority of patients with DRESS is head and neck oedema.
This is often most noticeable by looking at the ears. The face may be uniformly swollen, or have
a more leonine appearance
frank mucous membrane involvement is a rare. cheilitis is a common finding.
Pustules may be seen, but are more sparse than the sheets of pustules seen in AGEP
Clinical examination reveals lymphadenopathy in at least two sites in the majority of patients(the
nodes to be at least 2 cm in diameter to be considered clinically significant)
In haematological abnormalities:
1. Eosinophilia (MC) IL 5 levels, which stimulate eosinophil release, are elevated in DRESS .
‐
the protein contents of the eosinophil granules may have a pathogenetic role in the visceral
involvement in DRESS, being toxic to many tissues, including the liver .
2. Lymphocytosis with levels rising to >20 × 109 leukocytes/L.
Peripheral blood film: the presence of atypical lymphocytes, which are frequently present in
DRESS.
Leukopenia, lymphopenia (possibly virally induced) and thrombocytopenia have been noted
21.
Hepatic involvement:
liver- most common viscera to be involved, with both hepatocellular and obstructive patterns
of hepatitis reported. Between 70 and 95% of cases of DRESS demonstrate liver abnormalities
Although any drug has the potential to cause liver dysfunction in the context of DRESS, mostly
phenytoin, minocycline and dapsone cause more. Severity of involvement varies widely, from
mild and transient hepatitis, with alanine aminotransferase levels <250 iU/L, to fulminant hepatic
failure requiring liver transplantation
Liver dysfunction is the primary cause of mortality from DRESS
Renal involvement :
Is described in up to 10% of patients of DRESS.
certain drugs notably allopurinol cause a higher risk of kidney injury,. Any underlying renal
dysfunction may be exacerbated by the syndrome, and pre renal causes of kidney impairment
‐
such as dehydration from fever in the prodromal phase may contribute.
the patient may have haematuria, proteinuria and the presence of urinary eosinophils.
Histologically, interstitial nephritis is seen. Severe renal impairment analogous to the fulminant
liver failure is rare
22.
Cardiac involvement:
pericarditisand myocarditis
Cardiac complications are suggested by the presence of chest pain and dyspnoea.
Examination may reveal tachycardia, hypotension and signs of a pericardial and/or pleural
effusion.
ECG may demonstrate T wave abnormalities or other arrhythmias.
Echocardiogram may demonstrate a pericardial effusion, or reduced ejection fraction.
Cardiac enzymes such as creatine kinase MB fraction and troponin I may be elevated
a clinical variant of myocarditis known as acute necrotizing eosinophilic myocarditis (ANEM) has
been described in the context of DRESS. This is a severe form of myocarditis which carries a high
mortality (>50%). Diagnosis is suggested by findings on echocardiogram, such as extreme
impairment of ejection fraction and major systolic dysfunction
Pulmonary involvement :
Less common, but clinical symptoms of cough and dyspnoea should prompt examination and
investigation of the respiratory system, looking for pleural effusion, pleuritis or acute interstitial
pneumonitis . Lung function tests may reveal a reduced diffusion gradient
23.
Central nervoussystem involvement is rare
Gastrointestinal involvement in DRESS is rare, among which bloody diarrhoea, is the most
common presenting feature .In such cases an ulcerative colitis, with or without
eosinophilic infiltrate can found on endoscopic biopsy . Upper gastrointestinal tract
involvement, with eosinophilic oesophagitis and dysphagia has also been described
endocrine system involvement:
is more usual in the later phase of DRESS than the acute phase, with the thyroid gland
being most frequently involved.
Both hyper and hypothyroidism are seen in the convalescent phase, both of which may
‐
have a chronic course, and therefore regular monitoring of thyroid function for a year
after the acute event should be done.
Pancreatitis , pancreatic insufficiency presenting as type 1 diabetes are also described
Type 1 diabetes occurring following DRESS does not appear to be accompanied by islet
cell antibodies. (However the most common cause of diabetes in the context of DRESS is
that arising secondary to corticosteroid therapy administered for the disease)
24.
a. lymphadenopathy in≥2 sites, ≥1 cm. A maximum 1 point gained from lymphadenopathy
b. Eosinophilia: 10–19% of total white cell count = 1 point; ≥20% = 2 points (if total leucocytes <4 × 109/L,
an eosinophil count of 0.7–1.5 × 109/L will gain 1 point, an eosinophil count ≥1.5 × 109/L will score 2
points). Atypical lymphocytosis will gain 1 point.
c. Liver: transaminases >2 × upper limit of normal (ULN) on two successive dates or bilirubin × 2 ULN on 2
successive days or aspartate aminotransferase (AST), γ‐glutamyltransferase (GGT) and alkaline
phosphatase >2 × ULN on one occasion.
Renal: creatinine 1.5 × patient’s baseline.
Cardiac: echocardiographic evidence of pericarditis. Maximum of 2 points gained from internal organ
involvement.
d. ≥3 of the following performed and negative: hepatitis A, B and C; Mycoplasma/ chlamydia;
antinuclear antibody; blood culture (performed ≤3 days after hospitalization). A maximum of 1 point
gained for relevant negative serological tests.
25.
Differential diagnosis :
1.sepsis/infection, caused by virus or bacteria
2. Other SCAR Syndromes:
the pustules in AGEP tend to be predominantly flexural, whereas in DRESS they are unlikely
to be localized to these sites.
Epidermal loss, purpura and target lesions of the skin may be present in DRESS, all of which
may occur in EM, SJS or TEN.
One of the most helpful features in distinguishing DRESS from the other SCAR syndromes
is latency of onset of the eruption; this is classically shorter in AGEP (<5 days) and SJS/TEN (7–
10 days) than in DRESS, where the latency may be 2–6 weeks after drug ingestion
overlap syndromes do exist, and thus two diagnoses may not be mutually exclusive
3. Where exfoliative erythroderma is the presenting cutaneous feature of DRESS, this may
mimic the presentation of an acute severe eczema or psoriasis, or a cutaneous lymphoma
4. Where purpura and targets are present, the differential diagnosis of a systemic vasculitis
should be considered.
5. Angioimmunoblastic lymphoma is a rare differential
26.
Complications and comorbidities
‐ :
The most severe and life threatening complication of DRESS is fulminant liver failure,
‐
necessitating transplant or leading to death. Mortality has been estimated at 5–10%,
with hepatic failure being the predominant cause of death.
A delayed onset interstitial nephritis
‐
persistent interstitial pneumonitis
Thyroid dysfunction may supervene in the convalescent phase of DRESS.
Myocarditis, with associated cardiac insufficiency has also been described.
Autoimmune phenomena may arise following DRESS, including lupus erythematosus,
alopecia areata and autoimmune thyroid disease. The autoantibodies detected were
antinuclear antibody (ANA), antithyroglobulin antibody (ATGA) and antithyroperoxidase
antibody (ATPOA).
chronic exfoliative dermatitis.
27.
Disease course andprognosis:
The majority of patients with DRESS will recover fully, following withdrawal of the
culprit drug and management of the acute episode.
Poor prognostic markers :
1. The EM like
‐ presentation
2. cases of DRESS due to allopurinol and minocycline
3. haematological markers such as eosinophilia, pancytopenia and thrombocytopenia
as well elevated ferritin and elevated creatinine
4. Serum thymus and activation related chemokine (TARC) levels are a marker of
‐
disease severity,
28.
Suggested investigations indrug reaction with eosinophilia and systemic symptoms (DRESS) :
1. Basic laboratory screening during the acute phase
• CBC with differential, platelet count, peripheral smear for atypical lymphocytes
• BUN, creatinine, urinalysis, spot urine for protein : creatinine ratio
• LFTs, creatine kinase (CK), lipase, CRP
• TSH, free T4 (repeat at 3 months, 1 year, and 2 years)
• Fasting glucose (in anticipation of systemic corticosteroids)
2. Additional testing
• ECG, troponin T, baseline echocardiogram
• Quantitative PCR for HHV-6, HHV-7, EBV, CMV
• Wright stain of urine for eosinophilia (prior to instituting corticosteroids)
• ANA, blood cultures (exclusion criteria in RegiSCAR scoring system)
• If hemophagocytic lymphohistiocytosis suspected : ferritin, triglycerides, LDH, BM examination
3. Further testing based upon laboratory abnormalities or signs and symptoms
• Liver – PT, PTT, albumin • Renal – albumin, renal ultrasound (if laboratory abnormalities)
• Cardiac – ECG, troponin T, echocardiogram
• Neurologic – brain MRI • Pulmonary – CXR, PFTs • Gastrointestinal – endoscopy
29.
Management :
Themost important initial task once the diagnosis of DRESS is established is to identify and
exclude the culprit medication
In all cases, supportive care should be prioritized, placing the patient in a clinical area
equipped to provide an intensity of clinical care and monitoring appropriate to the severity
of disease. This may involve intravenous fluids, thermoregulation, catheterization to facilitate
fluid balance management and supplemental oxygen.
Skin directed therapy should be prescribed including topical emollient and, if appropriate,
‐
topical corticosteroid therapy.
The mainstay of active treatment is corticosteroid therapy, administered topically, orally or
intravenously. In refractory cases, or where the disease enters a chronic phase, recourse to
a steroid sparing agent such as ciclosporin may be required.
‐
Advice regarding the management of organ specific involvement should be sought from
‐
appropriate specialties, such as hepatology, cardiology, renal medicine, respiratory
medicine.
30.
First line:
Incases of limited severity with minimal cutaneous involvement, or where administration of
corticosteroid by other routes is contraindicated, the application of highly potent topical
steroids may suffice as treatment.
However, the majority of patients will require systemic corticosteroid therapy, either via the
oral route or the intravenous route, as guided by clinical state. Oral prednisolone of 1
mg/kg/day is recommended as initial treatment, with a tapering off period varying from 1
‐
to 3 months.
Where intravenous therapy is required, or where institution of oral therapy has failed
to produce a satisfactory clinical improvement, methylprednisolone is indicated (1 g/day
methylprednisolone for 3 days)
Second line
Cases of DRESS refractory to steroid treatment may require alternative agents like
Ciclosporin which is useful in patients where a protracted course of illness (e.g. with
persistent liver dysfunction or a chronic exfoliative dermatitis) supervenes.
The use of intravenous immunoglobulin (IVIg) as second line therapy has been described.
The rationale for IVIg is based on early observations that a fall in endogenous
immunoglobulins is seen in DRESS, and this has a permissive effect on virus reactivation
31.
Third line
Thisinclude treatments used in refractory cases of DRESS.
Plasmapharesis.
Alternative immunosuppressants such as cyclophosphamide may be used for their steroid‐
sparing effect.
Rituximab has been reported to have benefit in this setting.
Valganciclovir to combat virus reactivation
In cases of severe liver involvement, N acetylcysteine has been used as an adjunct to other
‐
treatments
Extracorporeal membrane oxygenation (ECMO) has been used in cases of cardiac
insufficiency secondary to myocarditis in DRESS
32.
Drug induced generalizedexfoliative
‐
dermatitis(Drug induced erythroderma
‐ )
Generalized exfoliative dermatitis (GED) is an adverse drug reaction characterized by
erythema and scaling affecting more than 90% of the body surface area.
Incidence and prevalence : GED accounts for 2-8% of all cutaneous adverse drug reactions
in hospitalized patients . Drug induced GED accounts for 5-40% of all erythroderma
‐
Pathophysiology:
GED is characterized by increased epidermal turnover, decreased transit time and increased
mitotic activity. a complex interaction of cytokines, chemokines and adhesion molecules is
involved.
Cases of benign exfoliative dermatitis (including drug induced cases) were found to have an
‐
overexpression of both Th1 and Th2 related chemokine receptors and respective ligands as
‐ ‐
opposed to a Th2 cytokine profile in Sézary syndrome .
Upregulation of adhesion molecules such as CD62L on keratinocytes may also facilitate the
hypersensitivity reaction through the recruitment of epidermal T cells and Langerhans
cells
Pathology :
The utility of histology in diagnosing drug induced GED remains limited. Correlation between
‐
pathological and clinical diagnosis of drug induced GED occurs in only 35% of cases
‐
Clinical features
History :
The onset of primary drug induced GED typically has an abrupt onset within days of the
‐
intake of the offending drug . However, in cases associated with DRESS, the latency from
drug initiation to the onset of rash occurs up to 12 weeks of drug initiation.
Presentation :
Patients present with generalized scaling and erythema associated with pruritus.
Constitutional symptoms such as malaise, hypothermia or fever may be present as well as
signs of lymphadenopathy, organomegaly and high output cardiac failure.
‐
The presence of fever has been found to be significantly associated with druginduced cases
Differential diagnosis :
This includes other causes of generalized exfoliative dermatitis, such as acute psoriasis,
eczema or cutaneous T cell lymphoma.
‐
Complications and co morbidities
‐ :
Include hypothermia, fluid and electrolyte imbalances, high output cardiac failure and
‐
sepsis from the impaired skin barrier. Long term sequelae of post inflammatory
‐ ‐
dyspigmentation may also occur.
35.
Disease course andprognosis :
GED arising from medications generally has the best prognosis and improves with
discontinuation of the offending drug.The exception being those associated with DRESS,
in which the cutaneous reaction may persist for weeks despite drug withdrawal.
Investigations :
Patch testing to determine drug causality in GED. However, positivity is related to the
type of drug tested. (Results are more likely to be positive when patch tested to
carbamazepine, pristinamycin, co trimoxazole,
‐ β‐lactams and diltiazem).
Management :
Identification and withdrawal of the offending drug.
Topical and systemic corticosteroids are indicated.
36.
Stevens–Johnson syndrome/toxic
epidermal necrolysis
Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are severe
mucocutaneous reactions, usually to drugs, characterized by epidermal loss and
multisite mucositis, accompanied by systemic complications, and may proceed to
multiorgan failure.
The two terms describe phenotypes within a severity spectrum, in which SJS is the less
extensive form and TEN is the more extensive. Both names are used to describe the
syndrome, thus: SJS/TEN (Lyell syndrome)
The incidence : of SJS/TEN is approximately one to two cases per million per year
Age : SJS/TEN occurs in all age groups including infants and children. There is an
increased incidence in the elderly.
There is an increased incidence in women, the female to male ratio being 2 : 1
Associated diseases : There is an increased risk of SJS/TEN in HIV infected individuals
‐ .
There is a suggested association with SLE, however an extensive form of acute bullous
LE can mimic TEN
37.
Classification of severity:
according to type of cutaneous lesion and extent of
maximal epidermal detachment :
1. •SJS is defined as: epidermal detachment less than
10% BSA, plus widespread purpuric macules or flat
atypical targets.
2. •Overlap SJS-TEN: detachment of 10–30% BSA, plus
widespread purpuric macules or flat atypical targets.
3. •TEN with spots: detachment greater than 30% BSA,
plus widespread purpuric macules or flat atypical
targets.
4. •TEN without spots: detachment greater than 30%
BSA, with loss of large epidermal sheets without
purpuric macules or target lesions.
38.
PATHOPHYSIOLOGY
A numberof medications can trigger widespread apoptosis of epidermal keratinocytes in
individuals with SJS or TEN, leading to skin blistering and denudation.
Theories proposed for this condition include:
(A) the medication might induce upregulation of FasL by keratinocytes constitutively expressing Fas,
leading to a death receptor-mediated apoptotic pathway;
(B) the drug might interact with MHC class I-expressing cells and then drug-specific CD8+ cytotoxic T
cells accumulate within epidermal blisters, releasing perforin and granzyme B that kill keratinocytes;
(C) drug-activated monocytes could secrete annexin A1, which induces necroptosis in keratinocytes
via binding to formyl peptide receptor 1 (FPR1);
(D) the drug may also trigger the activation of CD8+ T cells, NK cells and NKT cells to secrete granulysin,
with keratinocyte death not requiring cell contact. granulysin is the key mediator of apoptosis in SJS/
TEN.
Pro apoptotic molecules, including tumour necrosis factor
‐ ‐α, interferon‐γ, and inducible nitric oxide
synthase, are also involved in keratinocyte damage.
NOTE: IVIg contains antibodies against Fas that can block the binding of FasL to Fas
39.
Commonest drugs causingStevens–Johnson syndrome/toxic
epidermal necrolysis (SJS/TEN) :
•Allopurinol
•Carbamazepine
•Lamotrigine
•Nevirapine
•Oxicam non steroidal anti inflammatory drugs
‐ ‐
•Phenobarbital
•Phenytoin
•Sulfamethoxazole and other sulfa antibiotics
•Sulfasalazine
40.
Histopathology :
Thereis variable epidermal damage ranging from
individual cell apoptosis to confluent epidermal
necrosis
Keratinocyte necrosis is also seen in mucosal
biopsies.
Epidermal changes are associated with basal cell
vacuolar degeneration and subepidermal vesicle or
bulla formation
Adnexal structures such as sweat ducts and hair
follicles are occasionally involved.
Within the dermis, there is usually only a mild
perivascular infiltrate of lymphocytes and histiocytes.
Dermal eosinophils occur in the minority of cases
and, if present, tend to be few in number
41.
Causative organisms:
Inat least 15% of SJS/TEN cases a culprit drug is not identified.
In SJS, some cases, especially in children, appear to be triggered by infections, most
notably by Mycoplasma pneumoniae
Mycoplasma induced
‐ SJS (mostly children): characterized by a predominance of
mucous membrane involvement with little or no cutaneous lesions. This clinically atypical
form of SJS has been termed Mycoplasma pneumoniae-associated mucositis (MPAM)
Genetics:
a strong genetic predisposition to the development of carbamazepine induced
‐
SJS/TEN in individuals bearing HLA B*1502 and an association of HLA B*5801 with
‐ ‐
allopurinol induced SJS/TEN
‐
Genetic markers have the potential to be used as pharmacogenetic tests to identify
individuals at risk of SJS/TEN
42.
Clinical features
History :
A latent period occurs between initiation of the culprit drug and onset of
SJS/TEN. This latency is typically 7–10 days, but ranges from 5 to 28 days.
A history of malaise, fever and upper respiratory tract symptoms often
precedes the onset of the dermatosis by a few days (the prodrome).
The rash of SJS/TEN commonly develops on the face and chest initially and
disseminates widely over the ensuing days. Pruritus and cutaneous pain
accompany the skin signs.
Involvement of mucosal sites may occur before, after or simultaneously with
the dermatosis.
SJS/TEN involvement of the respiratory tract presents with cough, chest pain,
dyspnoea or haemoptysis; involvement of the bowel is characterized by
diarrhoea.
43.
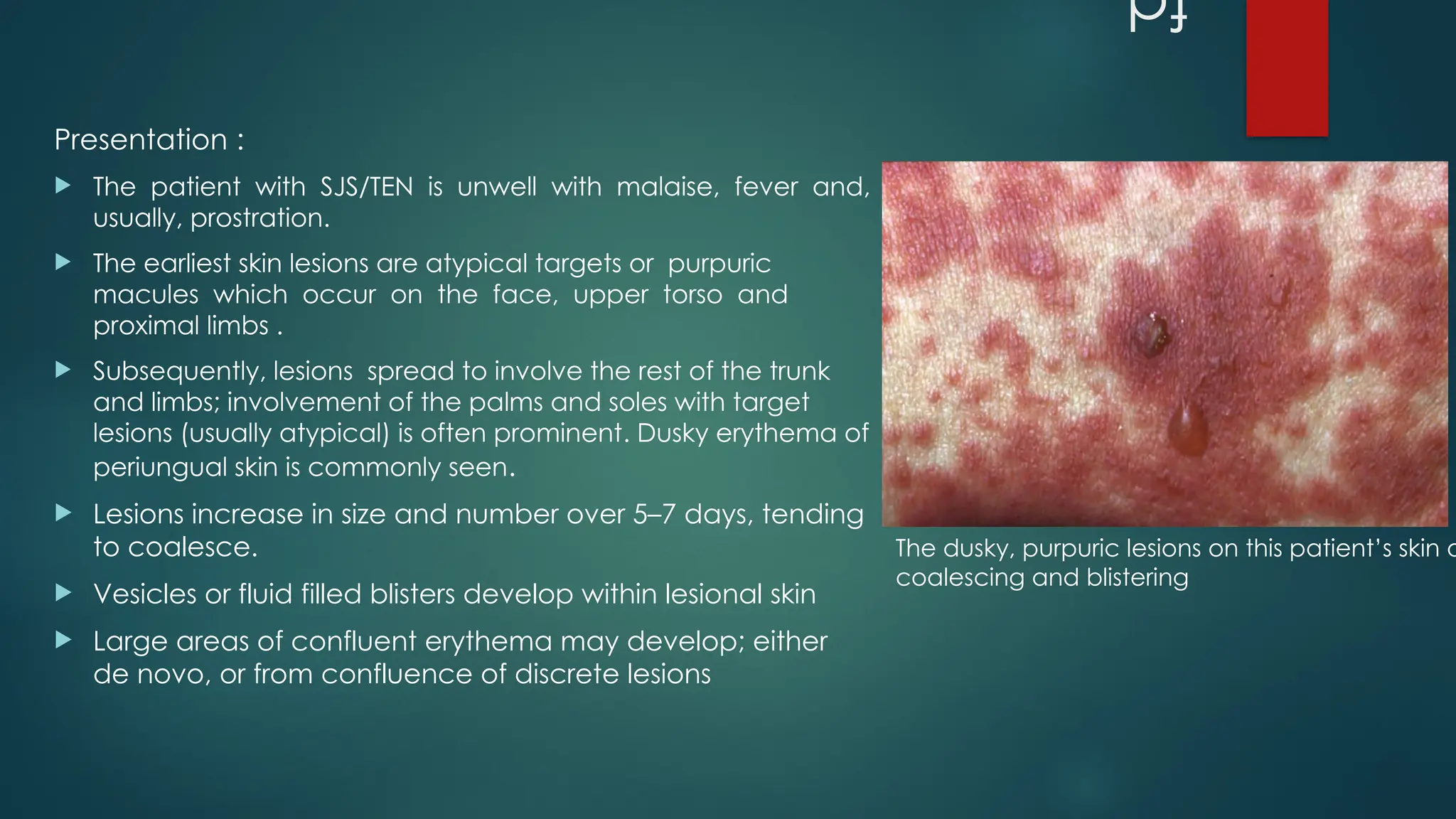
Presentation :
Thepatient with SJS/TEN is unwell with malaise, fever and,
usually, prostration.
The earliest skin lesions are atypical targets or purpuric
macules which occur on the face, upper torso and
proximal limbs .
Subsequently, lesions spread to involve the rest of the trunk
and limbs; involvement of the palms and soles with target
lesions (usually atypical) is often prominent. Dusky erythema of
periungual skin is commonly seen.
Lesions increase in size and number over 5–7 days, tending
to coalesce.
Vesicles or fluid filled blisters develop within lesional skin
Large areas of confluent erythema may develop; either
de novo, or from confluence of discrete lesions
The dusky, purpuric lesions on this patient’s skin a
coalescing and blistering
44.
Detachable epidermisshows a positive Nikolsky sign. It is a helpful
clinical indicator of epidermal necrolysis.
The combination of necrolytic blistering and shearing induced
‐
epidermal detachment will produce areas of denuded dermis which
readily bleed and can become secondarily infected.
Involvement of the mucous membranes of the eyes, mouth, nose and
genitalia is usually an early feature and leads to an erosive and
haemorrhagic mucositis.
Painful acute inflammation of the mucosal surfaces of the eye and
eyelids , causes visual impairment The ocular signs include chemosis,
conjunctivitis, pseudomembrane formation and corneal and
conjunctival epithelial defects
Compared to SJS, patients with TEN have more frequent but not more
severe acute ocular involvement
Oral involvement in SJS/TEN is characterized by painful mucosal
erythema with subsequent blistering and ulceration
May also extend to the oropharynx, larynx, respiratory tract and
oesophagus
45.
Similar changesto the vermillion of the lips progress to
the retention of adherent haemorrhagic crusts
Involvement of the urogenital tract in SJS/TEN is
characterized by mucosal erythema, blistering and
erosions During the acute phase, urogenital pain is
prominent and urinary dysfunction (dysuria or retention) is
common.
One fourth of SJS/TEN patients develop pulmonary
manifestations early in the disease characterized by
dyspnoea, increased respiratory rate and bronchial
hypersecretion. (Fibreoptic bronchoscopy reveals a
pattern of diffuse loss of bronchial epithelium in the
proximal airways, with evolving epithelial detachment
caused by epithelial necrosis)
SJS Erythema multiformemajor
(EMM)
Cause usually triggered by a drug,
rarely by an infection.
(Mycoplasma induced SJS
‐ )
mostly related to herpes
simplex virus reactivation,
Mycoplasma
pneumoniae and rarely to
drugs
cutaneous blistering with
epidermal detachment of
less than 10% body surface
area (BSA)
+ +
Cutaneous lesions Macular atypical targets
with predilection for the
trunk.
typical targets +/- Papular
atypical targets,
predominantly localized on
extremities and face
mucous membrane
involvement
+ +
Systemic symptoms Usually present:
Fever,Lymphadenopathy ,
Hepatitis ,Cytopenias
Usually present
• Fever
• Arthralgias
EMM showing Typical
target lesions are seen
as well as serous
crusting of the vermilion
lips and
eyelid margin. At the
margin of the serous
crusting of the lip, there
are two
zones of color with a
polycyclic outline
48.
Complications
Acute complications :
The commonest life threatening complication of acute SJS/TEN is septicaemia. The denuded dermis in SJS/TEN acts
‐
as a substrate for microbial colonization, initially by Staphylococcus aureus and later by Gram negative rods
‐
from the digestive flora, especially Pseudomonas aeruginosa. This may also lead to multiorgan failure
deranged thermoregulatory control leading to Hypothermia
Skin failure also results in considerable transcutaneous fluid losses, compounded by decreased oral fluid intake
due to disease involvement of the mouth.
Epidermal detachment of 50% BSA will lead to a water loss of 2–3 L/day from exudation and evaporation. Fluid
depletion can cause end organ hypoperfusion leading to acute kidney injury.
‐
Haematological complications : anaemia and leucopenia.
Abnormal liver function is typical during the early stage of the disease, but rarely leads to hepatic failure.
Hypoalbuminaemia usually occurs in TEN.
Hyperglycaemia may develop as a stress response in acute SJS/TEN.
Extensive epidermal detachment is accompanied by a greatly increased metabolic demand.
Epithelial necrolysis may occur in the bronchi during the acute phase of SJS/TEN resulting in bronchial erosions and
airway obstruction by sloughed epithelium. This occurs in up to 25% of patients and causes dyspnoea,
haemoptysis, increased bronchial secretion and hypoxaemia
Colonic involvement in SJS/TEN can occur rarely
49.
Long term complications
‐:
1. In the skin :
post inflammatory dyspigmentation
‐
cicatricial healing may develop in areas which were infected during the acute phase, at
sites of unrelieved pressure injury, and in circumstances where skin grafts were used
Eruptive melanocytic naevi occur occasionally in the recovery phase, more commonly in
children and young adults
Shedding of nails (onychomadesis) may occur due to nail matrix arrest; occasionally, there
is subsequent permanent anonychia
Involvement of the scalp in acute SJS/TEN is extremely unusual, however telogen effluvium
occurs in about 20% of patients in the post acute phase.
‐
Other skin complications include: pruritus, abnormal photosensitivity, abnormal sweating
and heterotopic ossification
50.
2. Long termocular sequelae
‐ :
are the most disabling complications of SJS/TEN.
Chronic complications include corneal and conjunctival ulceration and scarring, dry eye,
distichiasis, entropion, trichiasis and ocular surface failure
Corneal erosions and ulcers are perpetuated by the loss of limbal corneal stem cells, as
well as destruction of the conjunctival goblet cells, which impairs the tear film
In the conjunctiva, scarring of the fornix obstructs the ductal openings of lacrimal glands
thus aggravating ocular dryness.
Bulbar and forniceal cicatricial changes lead to symblepharon or ankyloblepharon
formation with limitation of ocular mobility and interference of the tear meniscus.
Scarring of the eyelid margin leads to ectropion, entropion and misdirected eyelashes.
Patients with chronic eye involvement require lifelong management for dryness,
conjunctival inflammation and ocular discomfort; many suffer permanent visual
impairment or blindness.
51.
3. long termoral complications
‐ :
Oral mucosal scarring can cause gingival synechiae resulting in food trapping and limitation of oral
mobility
A Sjögren like syndrome has been reported (ANA/Ro/ La negative) and is occur in up to 40% of
‐ ‐
survivors
4. Late complication of pulmonary involvement
is bronchiolitis obliterans, in which airway epithelial injury is followed by regeneration and scarring It leads
to severe airway obstruction and progressive dyspnoea. Most cases present 3–4 months after the acute
episode and are associated with a poor prognosis.
5. Long term complications in the gastrointestinal tract
‐
oesophageal stricture(rare)
Intestinal ulceration may occur in acute SJS/TEN and usually heals along with skin re epithelialization, in
‐
some patients small intestinal ulcers can be persistent causing diarrhoea and malabsorption.
Vanishing bile duct syndrome, characterized by cholestasis and histological loss of interlobular bile ducts
6. gynaecological complications
vaginal and introital adhesions may be associated with dyspareunia and rarely haematocolpos.
vaginal adenosis which is the replacement of non cornified vaginal epithelium with metaplastic
‐
epithelium of endocervical differentiation
7. psychological sequelae, including post traumatic stress disorder
‐
52.
Disease course andprognosis :
During the acute phase of SJS/TEN the extent of skin involvement increases over the first 5–7
days. With appropriate supportive therapy, and intensive skin/mucous membrane directed
‐
treatment , re epithelialization should start once the disease stops extending.
‐
Delayed healing will occur in the presence of skin sepsis, systemic complications, or if the
triggering agent (culprit drug) has not been removed. Uncomplicated re epithelialization
‐
will take 2–3 weeks to heal eroded areas.
The overall SJS/TEN mortality is about 22%; in SJS less than 10% of patients die from the
acute illness, while in TEN the mortality is approximately 30%
The cause of death in SJS/TEN is usually septicaemia induced multiorgan failure.
‐
The prognostic scoring system for SJS/TEN, is called SCORTEN (SCORe of Toxic Epidermal
Necrolysis), which uses seven clinical parameters to predict probability of hospital mortality
53.
The seven parametersused to calculate SCORTEN (SCORe of toxic
epidermal Necrolysis) :
•Age greater than 40 years
•Presence of malignancy
•Heart rate >120 beats/min
•Epidermal detachment >10% of BSA at admission
•Serum urea >10 mmol/L
•Serum glucose >14 mmol/L
•Bicarbonate level <20 mmol/L
SCORTEN (SCORe of Toxic Epidermal
Necrolysis) predicted mortality.
Number of
parameters
Predicted mortality
(%)
0 1.2
1 3.9
2 12.2
3 32.4
4 62.2
5 85.0
6 95.1
7 98.5
54.
Investigations
If SJS/TEN issuspected clinically, a set of investigations is needed to (a) substantiate the
diagnosis, (b) exclude other blistering dermatoses, and (c) identify any systemic
complications.
1. Important blood tests as listed below
2. A biopsy must be taken from lesional skin, just adjacent to a blister, for routine
histopathology. A second biopsy taken from peri blister lesional skin should be sent
‐
unfixed for direct immunofluorescence to exclude an immunobullous disorder.
3. At presentation, swabs should be taken from lesional skin and sent for bacteriology.
4. A chest X ray
‐ is mandatory.
5. Clinical photographs of the skin should be taken to show the type of lesion and extent of
involvement. The extent of erythema and the extent of epidermal detachment should
be recorded separately on a body map; for each parameter the percentage of BSA
involved should be estimated.
55.
Blood tests neededat presentation in Stevens–Johnson syndrome/toxic epidermal
necrolysis (SJS/teN):
•Full blood count
•Urea and electrolytes
•Amylase
•Bicarbonate
•Glucose
•Liver function tests
•Erythrocyte sedimentation rate
•C reactive protein
‐
•Coagulation studies
•Mycoplasma serology
•Antinuclear antibody and extractable nuclear antigen
•Complement levels
•Indirect immunofluorescence
56.
Treatment ladder
First line
Promptly discontinue any, and all, possible offending drugs
If epidermal loss is >10% BSA admit to a specialist unit (intensive care unit or burns unit)
Correct fluid and electrolyte imbalances
Heated environment
Nutritional regimen and Caloric replacement
Protect from secondary infections with topical antibiotic ointments
Periodic cultures of mouth, eyes, skin, sputum
Preventing/treating infection
Oral antacids and mouth care
Pulmonary toilet, if respiratory symptoms are seen
Adequate analgesia
Physical therapy to prevent contractures
Specialist skin care nursing is essential for delivery of topical therapy/dressings
If extensive denuded areas, use biological dressings or skin equivalents
Ophthalmology consult and good eye care
Urology consult if urethral inflammation
MANAGEMENT
57.
Second line Inthe early stages of the acute phase consider using:
1. •IVIG (0.5–1 g/kg daily for 3–4 consecutive days), or
2. •Systemic corticosteroid (e.g. prednisolone 0.5–1 mg/kg daily for 10 days, and tapered; or
IV methylprednisolone 500 mg on 3 consecutive days), or
3. •Ciclosporin (3 or 4 mg/kg/day in divided doses for 10 days, and tapered)
A latent period between the drug initiation and onset of SJS/TEN always occurs; a latency
of 7–10 days is typical, but this period can range from 5 to 28 days.
58.
Skin care:
1.Shearing forces applied to the skin during patient positioning, should be limited
2. If detached epidermis can be left in situ to act as a biological dressing for the
underlying dermis. In cases where bullae are prominent, blisters can be decompressed
by fluid aspiration and the blister roof retained to cover the underlying dermis
3. The intact skin should be cleansed each day by gentle irrigation with warmed sterile
water or sprayed with a weak solution of chlorhexidine (1/5000).
4. The whole skin, including denuded areas, should be treated with frequent applications
of a greasy emollient, such as 50% white soft paraffin with 50% liquid paraffin (50/50
WSP/LP)
5. The use of dressings on denuded areas in SJS/TEN will reduce fluid and protein loss, limit
microbial colonization, help pain control and accelerate re epithelialization
‐
59.
Mucosal care:
1.Proper Ocular hygiene , using ocular lubricant ,a broad spectrum topical antibiotic ,and if
needed a topical corticosteroid drops, supervised by an ophthalmologist, may reduce
ocular surface damage in the acute phase of SJS/TEN
2. Maintain oral hygiene , regular oral examination , Apply WSP ointment frequently to the
lips; protect ulcerated intra oral surfaces with a mucoprotectant mouthwash. Clean the
‐
mouth daily with warm saline mouthwashes or an oral sponge. Use an anti inflammatory
‐
oral rinse containing benzydamine hydrochloride every 3 h, and an antiseptic mouthwash
(e.g. chlorhexidine digluconate) twice per day. In the absence of secondary infection,
consider using a topical corticosteroid four times per day
3. Examine the uro genital tract regularly ,Use an emollient frequently. a topical
‐
corticosteroid cream with additional antimicrobial activity can be applied to the involved
but non eroded surfaces. Catheterizing all patients will prevent urethral strictures.
‐
60.
Enteral nutritionis preferable to parenteral nutrition to reduce peptic ulceration and limit
translocation of gut bacteria. In case of buccal mucositis naso gastric feeding with a
‐
silicone tube should be instituted.
During the early, catabolic phase of SJS/TEN 20–25 kcal/kg/day should be delivered, while
requirements in the recovery, anabolic phase increase to 25–30 kcal/kg/day
Prophylactic anticoagulation with low molecular weight heparin is necessary, unless
‐ ‐
contraindicated.
Neutropenia will increase the risk of sepsis and therefore administration of recombinant
human granulocyte– colony stimulating factor (G CSF) has been used to resist infectious
‐ ‐
complications . G CSF may also be immunomodulatory and enhance re epithelialization
‐ ‐
The detection of sepsis may also be indicated by a rise in CRP, a neutrophilia and an
increase in skin pain.


![Acute generalized exanthematous
pustulosis (Exanthemic pustular psoriasis /Toxic
pustuloderma /Pustular drug rash)
Incidence:1–5 per million per year
mean age of onset :56 years
male to female incidence ratio of 0.8
Associated diseases: infections such as Mycoplasma pneumoniae, coxsackievirus [8], parvovirus B19 and
cytomegalovirus (CMV) .
Mercury exposure and spider bites have also been associated
Pathophysiology:
1. Drug specific CD4+ and CD8+ cells are involved
‐
2. high level of CXCL8 ( a proinflammatory cytokine) production.
3. subtypes of T cells producing interleukin (IL) 8, a neutrophil attracting chemokine
‐ have also been
identified in the peripheral blood of patients with AGEP.These are important in the pathogenesis of the
sterile pustules seen in this disease process, by attracting neutrophils into the already oedematous skin and
creating pustules.
4. mutations in the IL36RN gene, which codes for the IL 36 receptor antagonist (IL 36Ra) are also involved
‐ ‐](https://image.slidesharecdn.com/scarppt-250303125505-537ee1ab/75/severe-cutaneous-adverse-drug-reactions-3-2048.jpg)















































































![Cutaneous Drug Reactions [Autosaved].ppt 2.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/cutaneousdrugreactionsautosaved-251014081902-3f3a2e35-thumbnail.jpg?width=640&height=640&fit=bounds)






















