Extrahepatic Biliary Apparatus
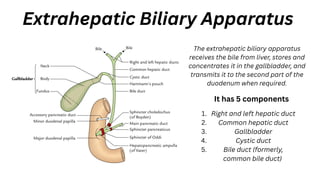
Theextrahepatic biliary apparatus
receives the bile from liver, stores and
concentrates it in the gallbladder, and
transmits it to the second part of the
duodenum when required.
It has 5 components
Right and left hepatic duct
1.
Common hepatic duct
2.
Gallbladder
3.
Cystic duct
4.
Bile duct (formerly,
common bile duct)
5.
4.
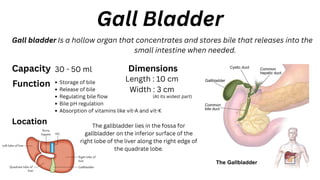
Gall Bladder
Gall bladderIs a hollow organ that concentrates and stores bile that releases into the
small intestine when needed.
Capacity 30 - 50 ml
Function Storage of bile
Release of bile
Regulating bile flow
Bile pH regulation
Absorption of vitamins like vit-A and vit-K
Location The gallbladder lies in the fossa for
gallbladder on the inferior surface of the
right lobe of the liver along the right edge of
the quadrate lobe.
Dimensions
Length : 10 cm
Width : 3 cm
(At its widest part)
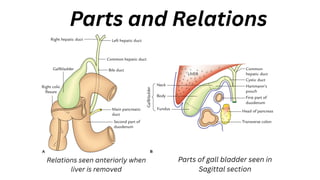
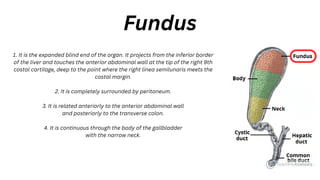
1. It isthe expanded blind end of the organ. It projects from the inferior border
of the liver and touches the anterior abdominal wall at the tip of the right 9th
costal cartilage, deep to the point where the right linea semilunaris meets the
costal margin.
2. It is completely surrounded by peritoneum.
3. It is related anteriorly to the anterior abdominal wall
and posteriorly to the transverse colon.
4. It is continuous through the body of the gallbladder
with the narrow neck.
Fundus
7.
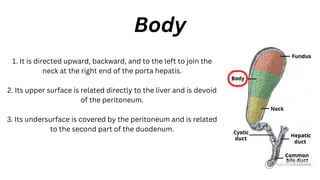
1. It isdirected upward, backward, and to the left to join the
neck at the right end of the porta hepatis.
2. Its upper surface is related directly to the liver and is devoid
of the peritoneum.
3. Its undersurface is covered by the peritoneum and is related
to the second part of the duodenum.
Body
8.
Neck
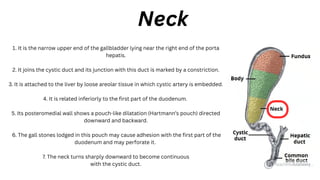
1. It isthe narrow upper end of the gallbladder lying near the right end of the porta
hepatis.
2. It joins the cystic duct and its junction with this duct is marked by a constriction.
3. It is attached to the liver by loose areolar tissue in which cystic artery is embedded.
4. It is related inferiorly to the first part of the duodenum.
5. Its posteromedial wall shows a pouch-like dilatation (Hartmann’s pouch) directed
downward and backward.
6. The gall stones lodged in this pouch may cause adhesion with the first part of the
duodenum and may perforate it.
7. The neck turns sharply downward to become continuous
with the cystic duct.
9.
Histology
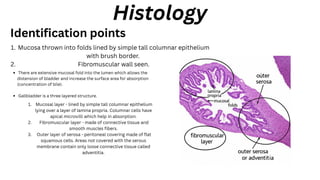
Mucosa thrown intofolds lined by simple tall columnar epithelium
with brush border.
1.
Fibromuscular wall seen.
2.
Identification points
There are extensive mucosal fold into the lumen which allows the
distension of bladder and increase the surface area for absorption
(concentration of bile).
Gallbladder is a three layered structure.
Mucosal layer - lined by simple tall columnar epithelium
lying over a layer of lamina propria. Columnar cells have
apical microvilli which help in absorption.
1.
Fibromuscular layer - made of connective tissue and
smooth muscles fibers.
2.
Outer layer of serosa - peritoneal covering made of flat
squamous cells. Areas not covered with the serous
membrane contain only loose connective tissue called
adventitia.
3.
10.
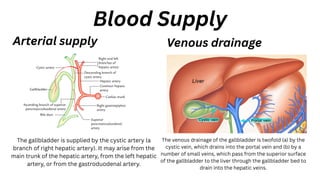
The gallbladder issupplied by the cystic artery (a
branch of right hepatic artery). It may arise from the
main trunk of the hepatic artery, from the left hepatic
artery, or from the gastroduodenal artery.
Blood Supply
Arterial supply
The venous drainage of the gallbladder is twofold (a) by the
cystic vein, which drains into the portal vein and (b) by a
number of small veins, which pass from the superior surface
of the gallbladder to the liver through the gallbladder bed to
drain into the hepatic veins.
Venous drainage
11.
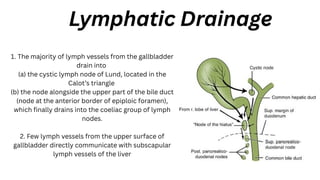
Lymphatic Drainage
1. Themajority of lymph vessels from the gallbladder
drain into
(a) the cystic lymph node of Lund, located in the
Calot’s triangle
(b) the node alongside the upper part of the bile duct
(node at the anterior border of epiploic foramen),
which finally drains into the coeliac group of lymph
nodes.
2. Few lymph vessels from the upper surface of
gallbladder directly communicate with subscapular
lymph vessels of the liver
12.
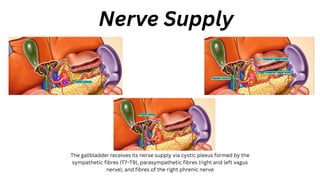
Nerve Supply
The gallbladderreceives its nerve supply via cystic plexus formed by the
sympathetic fibres (T7–T9), parasympathetic fibres (right and left vagus
nerve), and fibres of the right phrenic nerve
Congenital anomalies
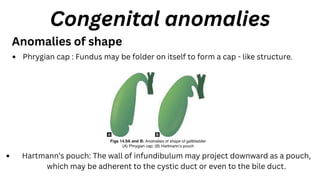
Anomalies ofshape
Phrygian cap : Fundus may be folder on itself to form a cap - like structure.
Hartmann’s pouch: The wall of infundibulum may project downward as a pouch,
which may be adherent to the cystic duct or even to the bile duct.
15.
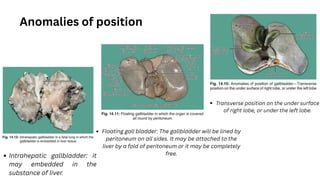
Floating gall bladder:The gallbladder will be lined by
peritoneum on all sides. It may be attached to the
liver by a fold of peritoneum or it may be completely
free.
Intrahepatic gallbladder: it
may embedded in the
substance of liver.
Anomalies of position
Transverse position on the under surface
of right lobe, or under the left lobe.
16.
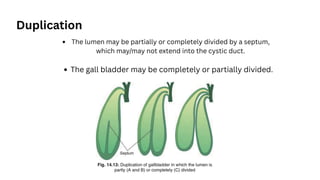
Duplication
The lumen maybe partially or completely divided by a septum,
which may/may not extend into the cystic duct.
The gall bladder may be completely or partially divided.
17.
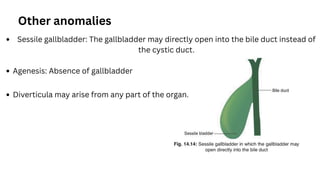
Other anomalies
Sessile gallbladder:The gallbladder may directly open into the bile duct instead of
the cystic duct.
Agenesis: Absence of gallbladder
Diverticula may arise from any part of the organ.
18.
References
Textbook of Anatomy(Vishram Singh): Abdomen and Lower Limb, Volume II, 2e
Inderbir Singh’s Human Embryology : 11th Edition