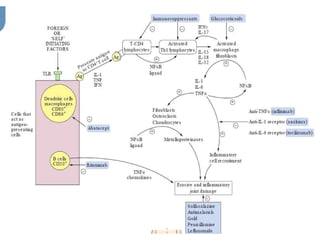
Rheumatoid arthritis (RA) is a chronic inflammatory disease characterized by polyarthritis, primarily affecting joints like the wrists and fingers, driven by immune-related cells and cytokines. Treatment includes disease-modifying antirheumatic drugs (DMARDs), both non-biological and biological, such as methotrexate and TNF-α inhibitors, which suppress inflammation but can have significant adverse effects. Corticosteroids and NSAIDs are commonly used for symptom relief but do not alter the disease course.











































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




