Jaw Bone Lesion Types, Causes, Symptoms and Treatments
•
1 like•1,036 views

Oral & Maxillofacial Surgery Fifth Year

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (14)
Similar to Jaw Bone Lesion Types, Causes, Symptoms and Treatments
Similar to Jaw Bone Lesion Types, Causes, Symptoms and Treatments (20)
More from IAU Dent
More from IAU Dent (20)
Recently uploaded
Recently uploaded (20)
Jaw Bone Lesion Types, Causes, Symptoms and Treatments
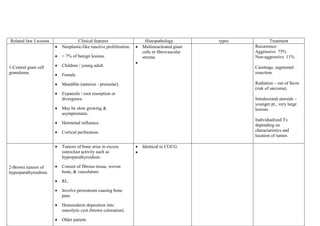
- 1. Related Jaw Lwsions < 7% of benign lesions. Children / young adult. Female. Mandible (anterior - premolar). 1-Central giant cell granuloma. Clinical features Neoplastic-like reactive proliferation. Expansile / root resorption or divergence. 2-Brown tumors of hyperparathyroidism. Tumors of bone arise in excess osteoclast activity such as hyperparathyroidism. Consist of fibrous tissue, woven bone, & vasculature. RL. Involve periosteum causing bone pain. Hemosiderin deposition into osteolytic cyst (brown coloration). Older patient. Radiation – out of favor (risk of sarcoma). Intralesional steroids – younger pt., very large lesions. Cortical perforation. Treatment Recurrence: Aggressive 75% Non-aggressive 11% Curettage, segmental resection. Hormonal influence. types May be slow growing & asymptomatic. Histopathology Multineucleated giant cells in fibrovascular stroma. Individualized Tx depending on charactaristics and location of tumor. Identical to CGCG.
- 2. 3-Cherubism. Genetic disorder (bilateral mandibular & maxillary intraosseous fibrous swellings). Young / with autosomal dominant inheritance. 4-Fibrous dysplasia Condition in which normal medullary bone is replaced by an abnormal fibrous connective tissue proliferation in which new, nonmaturing bone is formed. A genetic defect involving Gs-alpha proteins appears to underlie this process. Defect in the control of bone cell activity. Painless, expansile, dysplastic process of osteoprogenitor CT. Maxilla. Antrum, orbital floor involvement. Differential diagnosis: Indistinguishable histologically from Select up to 2 DD to compare CGCG. with Cherubism: Osteoclast-like - CGCG (mandible & multinucleated giant cells maxilla). - Primary hyperparathyroidism. - Ossifying fibroma. Cellular fibrous CT stroma contain foci of trabeculae of immature bone. Osteoclast-like multineucleated giant cell also in: 1- CGCG. 2- Giant cell tumor (osteoclastoma). 3- Fibro-osseous lesion. 4- Bone lesion of hyperparathyroidism. 5- Aneurismal bone cyst. 1- Monostatic: More common in jaw & cranium. (one bone) (much more common) 80% 2- Polystatic: McCune-Albright’s syndrome. Cutaneous pigmentation. Hyper-functioning endocrine glands. Precocious puperty. (more than one bone). If quiescent – contour excision (cosmesis or function). Accelerated growth or disabling functional impairment - surgical intervention
- 3. (globe displacement). With involvement of several adjacent bone (referred to as craniofacial fibrous dysplasia) The most common mandibular involvement is body portion. facial asymmetry may be initial presenting complaint. 1st & 2nd decades. Polystatic (females). 5-Ossifying fibroma “ground-glass appearance”. Poorly defined RL to uniformly radiopaque. True neoplasm of medullary jaws 3rd & 4th decades. Females. slow-growing, asymptomatic, & expansile lesion. Jaws & craniofacial bones.(mandibular premolar-molar area) expansion and thinning of the buccal and lingual cortical plates. Solitary. well-circumscribed RL (osteolysis) A mixed radiolucent-radiopaque juvenile (aggressive): younger than 15 years paranasal sinuses and periorbital bones the former lends itself to ready enucleation, while the latter can be admixed with surrounding tissues, making surgery more complicated. surgical removal using CURETTAGE OR ENUCLEATION.
- 4. image is seen when islands of tumor bone are densely calcified. Root displacement & tooth resorption Cementifying fibroma, and cemento-ossifying fibroma, are terms occasionally used when the bony islands in these lesions have a round or spheroidal shape. Other differential considerations are osteoblastoma, focal cementoosseous dysplasia, and focal osteomyelitis. Osteoblastoma is evident in a slightly younger age-group and is often characterized by pain. In addition, osseous trabeculae in these lesions are rimmed by abundant plump osteoblasts, and a central nidus may be evident. Periapical cemento-osseous dysplasia in posterior teeth may appear radiographically similar and require a biopsy to separate it from ossifying fibroma. Focal osteomyelitis is associated with a source of inflammation and is possibly accompanied by pain and swelling. Distinguishing between ossifying fibroma and fibrous dysplasia is the primary diagnostic challenge. Both lesions may exhibit similar clinical, radiographic, and microscopic features. The most helpful feature in distinguishing the two is the well circumscribed radiographic appearance of ossifying fibroma and the ease with which it can be separated from normal bone. In most cases the well defined appearance of ossifying fibroma is evident radiographically. Historically, differentiating the two lesions was based primarily on histologic criteria. Fibrous dysplasia was reported to contain only woven bone, without evidence of osteoblastic rimming of bone. The presence of more mature lamellar bone was believed to be characteristic of ossifying fibroma Done by/ Mahdi 207 for ever دعواتكم شباب