Regional anesthesia is very important part of anesthesia practice now.
Its increasingly practiced worldwide and is especially providing safe practice for patients having comorbidities.
Introduction
Regional anesthesiainvolves injection of local anesthetic
agents around nerves in the peripheral or central nervous
system to achieve reversible removal of nerve conduction and
pain senses in the corresponding innervated tissue without
causing loss of consciousness.
4.
Introduction
Regional anesthesiahas a very interesting long history,
initially preferred over general anesthesia because of
safety concerns.
The initial enthusiasm retreated with new general
anesthetic drugs and anesthetic adjuvants in the 1930s to
1950s.
Introduction of long-acting local anesthetics and
development of techniques for their safe use in the last
quarter of the century resurrected the fortunes of
regional anesthesia.
5.
Introduction
Nowadays insteadof competing, general and regional anesthesia
are complementing each other as a part of perioperative
management.
It is commonly believed that regional anesthesia is more
reliable than general anesthesia, especially among elderly
patients, a difference has also been demonstrated between
the two anesthesia types in terms of mortality and morbidity
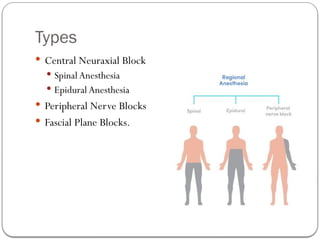
Central Neuraxial Block
CNB involves administration
of drugs in the epidural or
subarachnoid space for
anesthesia or analgesia of the
respective spinal cord section.
It is the oldest and most
commonly used regional
block technique.
8.
Central Neuraxial Block
The fact that epidural anesthesia can be
applied to a specific part of the spinal cord,
makes it useful for procedures where only a
segment of the cord needs to be anesthetized,
for example Cervical,Thoracic, Upper
Lumbar (for labour), and Caudal blocks.
Moreover the placement of catheter in the
epidural space makes prolonged
anesthesia/analgesia possible.
9.
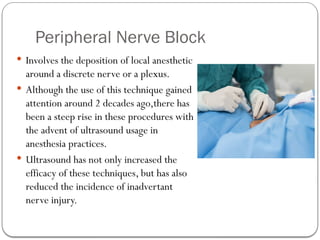
Peripheral Nerve Block
Involves the deposition of local anesthetic
around a discrete nerve or a plexus.
Although the use of this technique gained
attention around 2 decades ago,there has
been a steep rise in these procedures with
the advent of ultrasound usage in
anesthesia practices.
Ultrasound has not only increased the
efficacy of these techniques, but has also
reduced the incidence of inadvertant
nerve injury.
10.
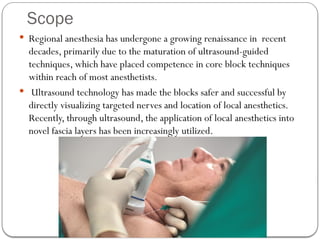
Scope
Regional anesthesiahas undergone a growing renaissance in recent
decades, primarily due to the maturation of ultrasound-guided
techniques, which have placed competence in core block techniques
within reach of most anesthetists.
Ultrasound technology has made the blocks safer and successful by
directly visualizing targeted nerves and location of local anesthetics.
Recently, through ultrasound, the application of local anesthetics into
novel fascia layers has been increasingly utilized.
11.
Scope
Frequency ofuse is increasing due to advantages over general
anesthesia
Avoidance of airway manipulation
Reduced doses and side effects of systemic drugs
Lower postoperative nausea and vomiting
Faster recovery time and early mobilization.
Significantly lower pain levels after surgery.
Shortened hospital stay
12.
Scope
For patientswith severe systemic disease, regional anesthesia
offers a safe alternative to general anesthesia.
13.
Scope
Some verycommon uses of regional anethesia are
In patients with Pulmonary pathologies such as
Consolidation
Diffuse lung disease
Inflammatory pathology
In patients with compromised hemodynamics
Upper and Lower Extremity Surgeries
Lower Abdominal and Pelvic Surgeries
Postoperative pain control
Treat certain chronic pain conditions
14.
Prospects
Fascial PlaneBlocks
Advances in Safety
Post operative pain management
Regional Anesthesia; Beyond Pain management
Acute Perioperative Pain Services
Training andAcademics
15.
Prospects
• Fascial planeblocks
Rise in popularity of regional anesthesia techniques that involve
an injection of local anesthetic into fascial planes rather than
directly around discrete nerves
Fascial plane blocks have found particular application in truncal
analgesia as simpler and safer alternatives to thoracic epidural
and paravertebral blockade
16.
Prospects
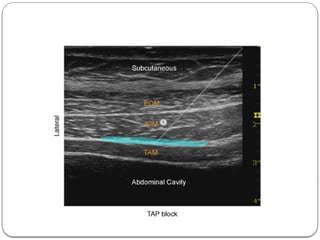
Fascial planeblocks
The transversus abdominis plane (TAP) block was the first to
enter mainstream practice, beginning as a surface landmark
guided technique and evolving into what is now known as the
lateral ultrasound-guided TAP block.
As the understanding of abdominal wall anatomy and
innervation advanced, variants on the lateral ultrasound-guided
TAP block approach developed, including the subcostal and
posteriorTAP blocks .
18.
Prospects
Fascial planeblocks
The site of actual injection into the TAP plane determines the
area of abdominal wall coverage
Thus the clinical indication and expected efficacy forTAP
blocks will depend on the specific approach being employed
Although TAP blocks have not replaced thoracic epidurals for
analgesia in major abdominal surgery, the evidence indicates
they are modestly effective with fewer side-effects than
epidurals, particularly hypotension.
19.
Prospects
Fascial planeblocks
Other ultrasound-guided fascial plane blocks such as the
rectus sheath, erector spinae plane (ESP) and
quadratus lumborum(QL) blocks may soon supersede
TAP block in its role as a simpler alternative to epidural
analgesia.
20.
Prospects : AdvancesIn Safety
Adoption of ultrasound guidance has contributed to the safety
of regional anesthesia, particularly due to the reduced risk of
local anesthetic systemic toxicity following peripheral nerve
blockade
This can be attributed to associated reductions in minimum
local anesthetic dose requirements and accidental vascular
puncture.
21.
Prospects
Advances InSafety
A similar impact of ultrasound guidance on the risk of
neurological complications following regional anesthesia has
yet to be conclusively demonstrated
However, this is unsurprising given the multifactorial etiology
and relatively low incidence of peri-operative peripheral nerve
injury.
22.
Prospects
Advances InSafety
Advances in regional anesthesia in this regard pertain primarily
to both an increased understanding of the micro architecture of
nerves and their surrounding tissues, as well as the ability to be
more selective about where we place the needle tip and deposit
drugs in relation to the nerve.
There has been a push for safer approaches to regional
anesthesia techniques, particularly in the brachial plexus, that
involve placing the needle or catheter tip further away from
target nerves
23.
Prospects
Advances InSafety
At the same time, the recognition that ultrasound-guided
regional anesthesia is a relatively complex procedure has led to
a greater focus on developing effective teaching strategies and
competency assessment tools.
It is likely that a structured educational approach, utilising
defined task metrics, will improve learner performance
24.
Prospects: Postoperative Pain
There is growing recognition of the need to reevaluate opioid
use as a mainstay of anesthesia and acute pain management
Regional anesthesia has always had a role to play in
perioperative opioid requirements, but it should no longer
be seen as merely an alternative to general anesthesia, rather
a complement to an overall multimodal anesthetic strategy
25.
Prospects
Postoperative Pain
Regional anesthesia may also contribute to a reduced risk of
persistent postoperative pain in a variety of clinical settings,
including breast surgery, thoracotomy and caesarean section.
Optimal efficacy for management of both acute and chronic
postoperative pain is likely to be obtained with pre-incisional rather
than postoperative nerve blockade and in combination with other
perioperative multimodal analgesic strategies.
This speaks to the importance of integrating regional anesthesia and
general anesthesia where indicated, rather than regarding them as
‘either/or’ options.
26.
Regional Anesthesia: BeyondAcute Pain
Management
The potential benefits of peri-operative regional anesthesia
extend beyond acute pain relief.
In total hip and knee arthroplasty, several large retrospective
studies have shown that, when compared with general
anesthesia, neuraxial anesthesia is associated with a reduction
in
patient mortality
major morbidity (e.g. pulmonary complications, transfusion
requirements) and
economic outcomes such as length of hospital stay.
27.
Prospects:
Acute Perioperative PainService
Established as a relatively new but important concept and
service in clinical patient care.
There is growing evidence of the multiple benefits of a
dedicatedAPPS, especially pertaining to patients at higher
risk of poorly controlled postoperative pain.
Importance of the perioperative pain management
continuity of care, consisting of preoperative pain evaluations
and post-discharge follow-up in an outpatient pain
management setting, in coordination with the primary teams.
28.
Prospects
Acute PerioperativePain Service
The APPS is becoming the clinical standard of care for
managing postoperative pain, and its role continues to expand
worldwide
29.
Prospects: Training &Academics
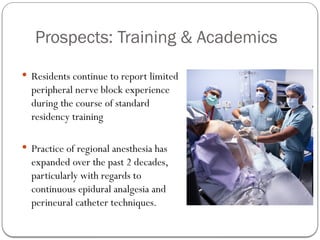
Residents continue to report limited
peripheral nerve block experience
during the course of standard
residency training
Practice of regional anesthesia has
expanded over the past 2 decades,
particularly with regards to
continuous epidural analgesia and
perineural catheter techniques.
30.
Prospects
Training
Thebenefits of regional anesthesia with respect to postoperative
analgesia, decreased nausea and vomiting, and patient safety is
increasingly realized by surgeons as well.
However, resident training in regional anesthesia and analgesia
techniques may not be fully concordant with the perception of
increased demand.
31.
Prospects
Training
Thereis a need to develop method of increasing exposure of
residents to peripheral nerve block procedures.
To formulate guidelines for regional anesthesia fellowship
training and develop post fellowship programs for regional
anesthesia training.