Downloaded 802 times




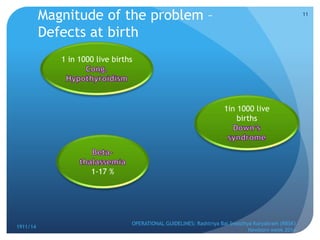
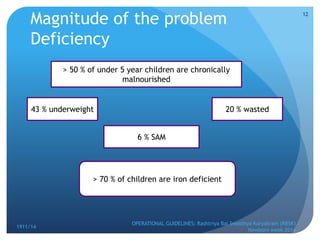
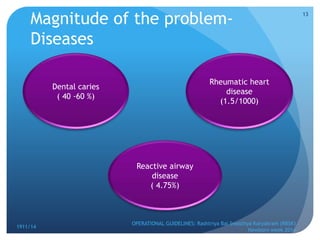
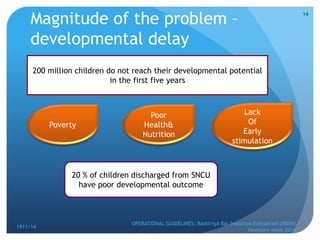
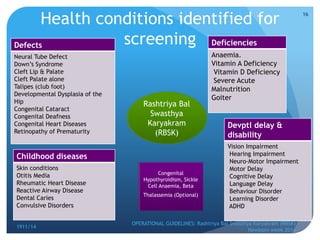

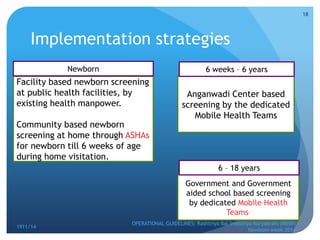
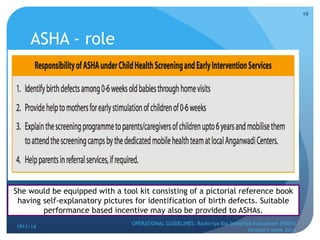

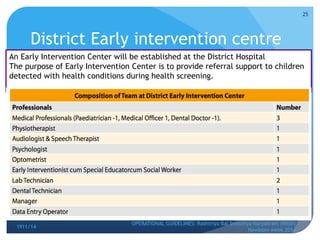
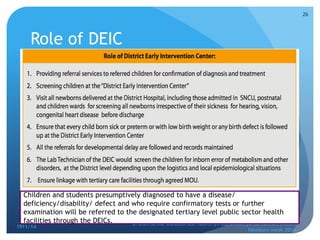
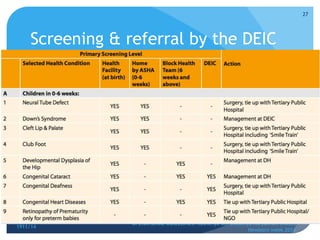
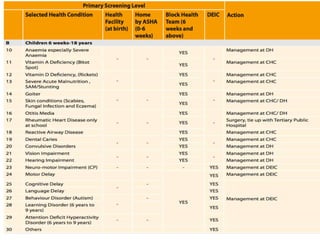



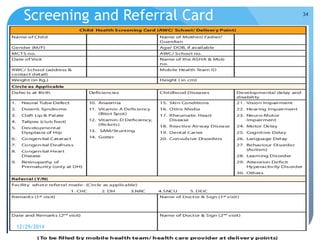
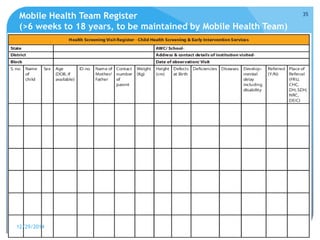
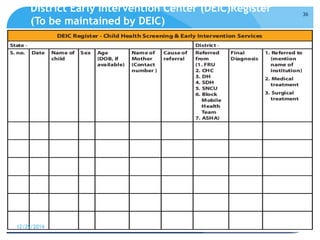
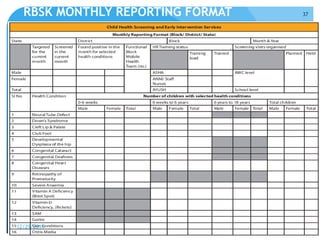


Rashtriya Bal Swasthya Karyakram (RBSK) or Child Health Screening and Early Intervention Services is an Indian government program that aims to screen and provide early intervention services for children from birth to 18 years. It focuses on screening for 30 health conditions including defects, diseases, deficiencies, and developmental delays. Mobile health teams screen children in anganwadi centers and schools twice a year. Children detected with issues are referred to District Early Intervention Centers for confirmation of diagnosis and further management. The program aims to improve child health through early detection and management of conditions not previously addressed.














































