Protein synthesis inhibitors
Presenter:Dr Umesh Kumar Maurya
Department of Pharmacology & Therapeutics
King George’s Medical University
Lucknow, Uttar Pradesh, India.
2.
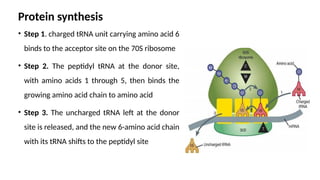
Protein synthesis
• Step1. charged tRNA unit carrying amino acid 6
binds to the acceptor site on the 70S ribosome
• Step 2. The peptidyl tRNA at the donor site,
with amino acids 1 through 5, then binds the
growing amino acid chain to amino acid
• Step 3. The uncharged tRNA left at the donor
site is released, and the new 6-amino acid chain
with its tRNA shifts to the peptidyl site
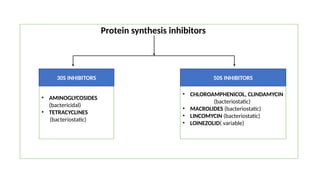
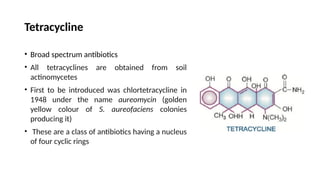
Tetracycline
• Broad spectrumantibiotics
• All tetracyclines are obtained from soil
actinomycetes
• First to be introduced was chlortetracycline in
1948 under the name aureomycin (golden
yellow colour of S. aureofaciens colonies
producing it)
• These are a class of antibiotics having a nucleus
of four cyclic rings
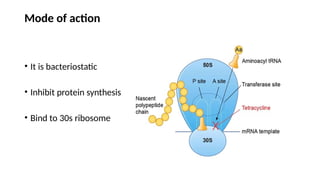
Mode of action
•It is bacteriostatic
• Inhibit protein synthesis
• Bind to 30s ribosome
7.
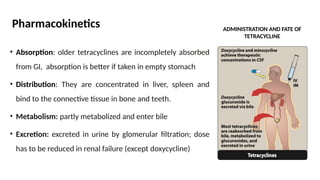
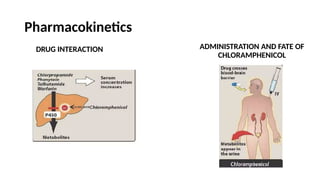
Pharmacokinetics
• Absorption: oldertetracyclines are incompletely absorbed
from GI, absorption is better if taken in empty stomach
• Distribution: They are concentrated in liver, spleen and
bind to the connective tissue in bone and teeth.
• Metabolism: partly metabolized and enter bile
• Excretion: excreted in urine by glomerular filtration; dose
has to be reduced in renal failure (except doxycycline)
ADMINISTRATION AND FATE OF
TETRACYCLINE
Resistance to Tetracycline
Resistanceto tetracyclines develops slowly in a graded manner
The three main resistance mechanisms are:
1. Concentrating mecha
nism becomes less efficient or the bacteria acquire capacity
to pump it out
2. Plasmid mediated synthesis of a ‘protection’ protein which protects the
ribosomal binding site from tetracycline
3. Enzymatic inactivation of tetracyclines
11.
Chloramphenicol
• Chloramphenicol, anantibiotic produced
by Streptomyces venezuelae
• It is a yellowish white crystalline solid, aqueous
solution is quite stable, stands boiling, but
needs protection from light
• The nitrobenzene moiety of chloramphenicol is
probably responsible for the antibacterial
activity as well as its intensely bitter taste
12.
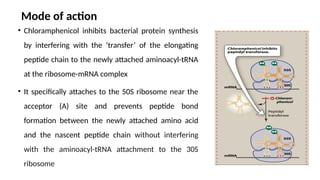
Mode of action
•Chloramphenicol inhibits bacterial protein synthesis
by interfering with the ‘transfer’ of the elongating
peptide chain to the newly attached aminoacyl-tRNA
at the ribosome-mRNA complex
• It specifically attaches to the 50S ribosome near the
acceptor (A) site and prevents peptide bond
formation between the newly attached amino acid
and the nascent peptide chain without interfering
with the aminoacyl-tRNA attachment to the 30S
ribosome
Resistance to Chloramphenicol
•Resistance to chloramphenicol is usually caused
by a plasmid-encoded acetyltransferase that
inactivates the drug
• Resistance can also result from decreased
permeability and ribosomal mutation
• Acetylated derivatives of chloramphenicol fail to
bind to bacterial ribosomes
Macrolides
• Characterized bya macrocyclic lactone ring (usually containing 14 or 16 atoms)
to which deoxy sugars are attached
• Erythromycin (first member) was discovered in 1950 from metabolic products
of a strain of streptomyces erythraeus
• Clarithromycin and azithromycin are semisynthetic derivatives of erythromycin
18.
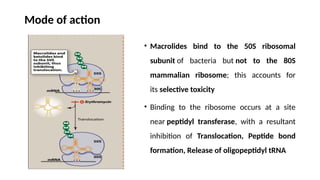
Mode of action
•Macrolides bind to the 50S ribosomal
subunit of bacteria but not to the 80S
mammalian ribosome; this accounts for
its selective toxicity
• Binding to the ribosome occurs at a site
near peptidyl transferase, with a resultant
inhibition of Translocation, Peptide bond
formation, Release of oligopeptidyl tRNA
19.
Antimicrobial Activity
• Erythromycinusually is bacteriostatic but may be bactericidal in high
concentrations against susceptible organisms
• The antibiotic is most active in vitro against aerobic gram-positive cocci and
bacilli
• In addition, Campylobacter, Legionella, Branhamella catarrhalis, Gardnerella
vaginalis, and Mycoplasma, that are not affected by penicillin, are highly
sensitive to erythromycin
20.
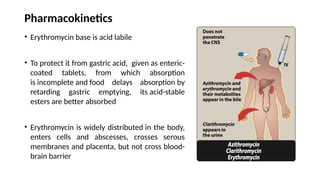
Pharmacokinetics
• Erythromycin baseis acid labile
• To protect it from gastric acid, given as enteric-
coated tablets, from which absorption
is incomplete and food delays absorption by
retarding gastric emptying, its acid-stable
esters are better absorbed
• Erythromycin is widely distributed in the body,
enters cells and abscesses, crosses serous
membranes and placenta, but not cross blood-
brain barrier
Therapeutic Applications ofMacrolides
1. Respiratory tract infections: community-acquired pneumonia
(CAP) pharyngitis, sinusitis, bronchitis diphtheria
2. Sexually transmitted infections: chlamydial infections ,chancroid and syphilis
3. Gastrointestinal infections: campylobacter enteritis, helicobacter pylori
eradication
4. Pertussis (whooping cough)
5. Prophylaxis in immunocompromised patients: MAC (mycobacterium avium
complex) infection in AIDS
23.
Lincomycin & Clindamycin
Classification:
•Lincomycin – natural lincosamide (rarely used now)
• Clindamycin – semisynthetic derivative of lincomycin (more commonly used)
Mechanism of Action:
• Inhibits bacterial protein synthesis by binding to the 50S ribosomal subunit
• Bacteriostatic (can be bactericidal at high concentrations)
24.
Antibacterial Spectrum:
• Goodactivity against Gram-positive cocci (including Streptococci, Staphylococci)
• Active against anaerobes – especially Bacteroides fragilis
• Not effective against aerobic Gram-negative bacilli
25.
Therapeutic Uses (mainlyClindamycin):
1.Anaerobic infections – especially intra-abdominal, pelvic, and dental infections
2.Aspiration pneumonia
3.Skin and soft tissue infections by Gram-positive cocci
4.Toxoplasmosis in combination with pyrimethamine
5.Prophylaxis of endocarditis in penicillin-allergic patients undergoing dental
procedures
6.Topical use in acne vulgaris (Clindamycin gel/lotion)
26.
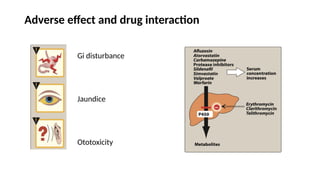
Adverse Effects:
• Diarrhoea
•Pseudomembranous colitis due to Clostridioides difficile overgrowth
• Rashes, liver dysfunction, neutropenia
27.
Linezolid
Classification:
• Oxazolidinone classof synthetic antibacterial agents
Mechanism of Action:
• Inhibits bacterial protein synthesis by binding to 23S rRNA of 50S ribosomal
subunit, preventing formation of the initiation complex
• Bacteriostatic against most organisms, but bactericidal against Streptococcus
pneumoniae
28.
Spectrum of Activity:
•Active against resistant Gram-positive organisms:
• MRSA (Methicillin-resistant Staphylococcus aureus)
• VRE (Vancomycin-resistant enterococci)
• Penicillin-resistant pneumococci
• Not effective against Gram-negative bacteria
29.
Therapeutic Uses:
1.Serious infectionscaused by resistant Gram-positive cocci
1. MRSA infections
2. VRE infections
3. Nosocomial pneumonia
4. Skin and soft tissue infections
2.Off-label use – drug-resistant TB (MDR-TB, XDR-TB)
30.
Adverse Effects:
• Myelosuppression(esp. thrombocytopenia on prolonged use)
• Peripheral and optic neuropathy
• Lactic acidosis
• Serotonin syndrome (with SSRIs/MAOIs – Linezolid is a weak MAO inhibitor)







![Protein synthesis inhibitors [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/proteinsynthesisinhibitorsautosaved-190403091041-thumbnail.jpg?width=640&height=640&fit=bounds)











































