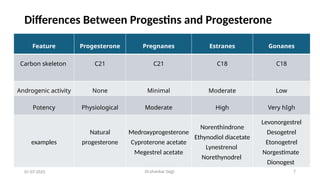
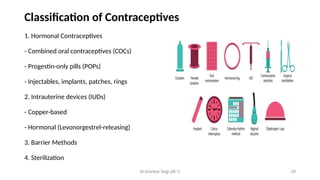
this ppt details about progesterone right from it's discovery to it's large scale synthesis via marker's degradation. structure activity relationship of all progesterone derivatives, it' s newer applications in postpartum depression in the form of Brexanolol etc.. also the research going on this topic. contraceptives are covered, mainly pharmacotherapy of contraception, newer emerging tools for contraception.