Downloaded 123 times

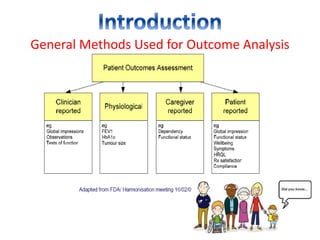


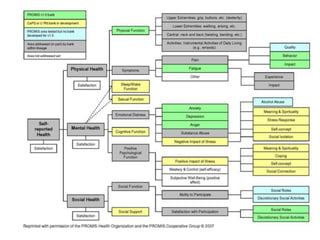
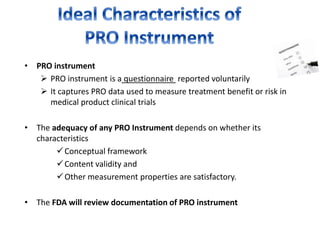
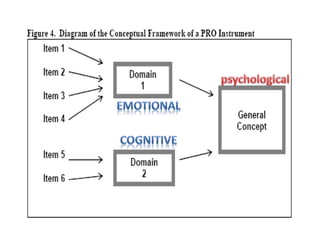
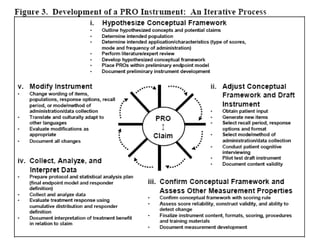
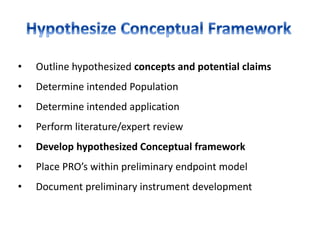
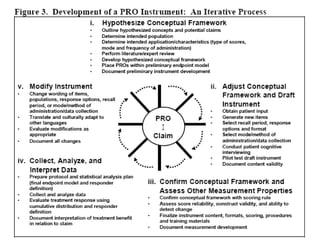

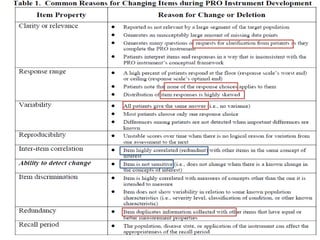
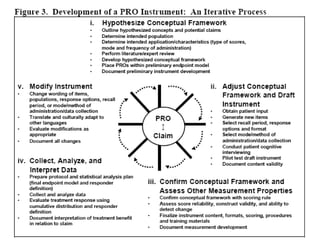
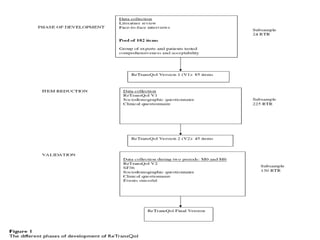


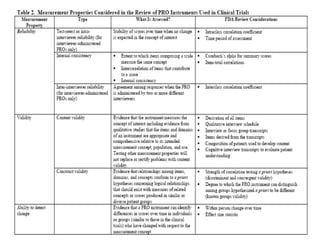


This document discusses patient-reported outcome (PRO) measures and developing PRO instruments. It covers: - Common diseases where PROs are used like Parkinson's and rheumatoid arthritis - Applications of PROs in clinical trials, medical practice, and economic evaluations - Developing a conceptual framework, ensuring content validity, and evaluating reliability - Modifying existing PRO instruments or developing new ones for specific populations like children













































![[Inf 295] week 6 parul seth patient-reported outcomes as a source of evidence...](https://cdn.slidesharecdn.com/ss_thumbnails/inf295week6parulsethpatient-reportedoutcomesasasourceofevidenceinoff-labelprescribing-131107002627-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































