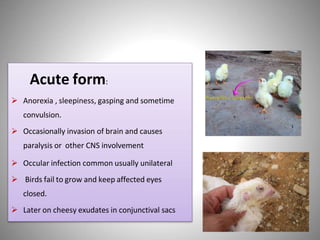
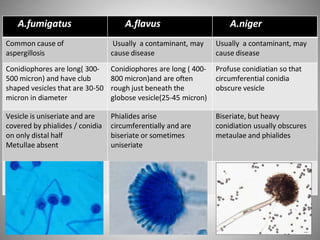
This document discusses Aspergillosis, a fungal infection caused by the genus Aspergillus. It has both acute and chronic forms that can infect the sinuses, lungs, and other organs of birds and mammals. The most common causative species are A. fumigatus, A. flavus, and A. niger. Aspergillosis is typically treated with antifungal medications like voriconazole, though treatment can be difficult. Control involves maintaining dry, clean living conditions and avoiding exposure to soil or dust to prevent spore transmission.