Introduction
• These drugsare usually effective in treatment of
mania and there the word antimanic is often used to
describe them.
• As these drugs are effective to manage mood
swings in bipolar disorder, the better term is mood-
stabilizing agent
• The most commonly used mood stabilizing agents
include lithium, valproate, carbamazepine and
lamotrigine, though there are several other
experimental mood stabilizers such as
oxacarbazepine.
4.
Definition
• Antimanic drugor Mood Stabiliser is
a psychiatric pharmaceutical drug
used to treat mood disorders
characterized by intense and
sustained mood shifts, typically
bipolar type I and type II.
Lithium
• Lithium isan element (Atomic number 3 and
Atomic weight 7) which is the smallest alkali ion.
• The element was discovered in 1817 by Arfuedson.
• Since then, it has been used for treatment of gout
and for salt replacement in cardiac disease, but its
use was restricted due to fatal toxicity.
7.
Contd…
• It wasrediscovered in 1949 by John Cade, for
use in treatment of mania but its potential went
unrecognized as it was discovered in Australia,
• Mogen Schou in 1957 had to rediscover it yet
again before it became popular as a treatment of
mania
Pharmacokinetics
• Lithium isvery rapidly absorbed from the
gastrointestinal tract.
• The peak serum levels occur between 30 minutes to
3 hours. The absorption is virtually complete in
about 8 hours.
• The maximum levels occur in thyroid (3-5 times
serum level), saliva (two times), milk (0.3-1.0 times)
and CSF (0.4 times).
.
11.
Contd…
• The steadystate levels are achieved in
about 7 days.
• There is no metabolism of lithium in body
and it is excreted almost entirely by the
kidneys
Contd…
• It stabilizesthe cell membrane, along with Ca++ and
Mg++.
• It decreases the Ca++ mobilisation from the
intracellular pools by ITP ( inositol-triphos phate)-
dependent Ca++ channels (II messenger system).
• It interferes with the phosphatidyl-inositol cycle by
blocking the conversion of IMP (inositol
monophosphate) to inositol, by inositol
monophosphate phosphatase.
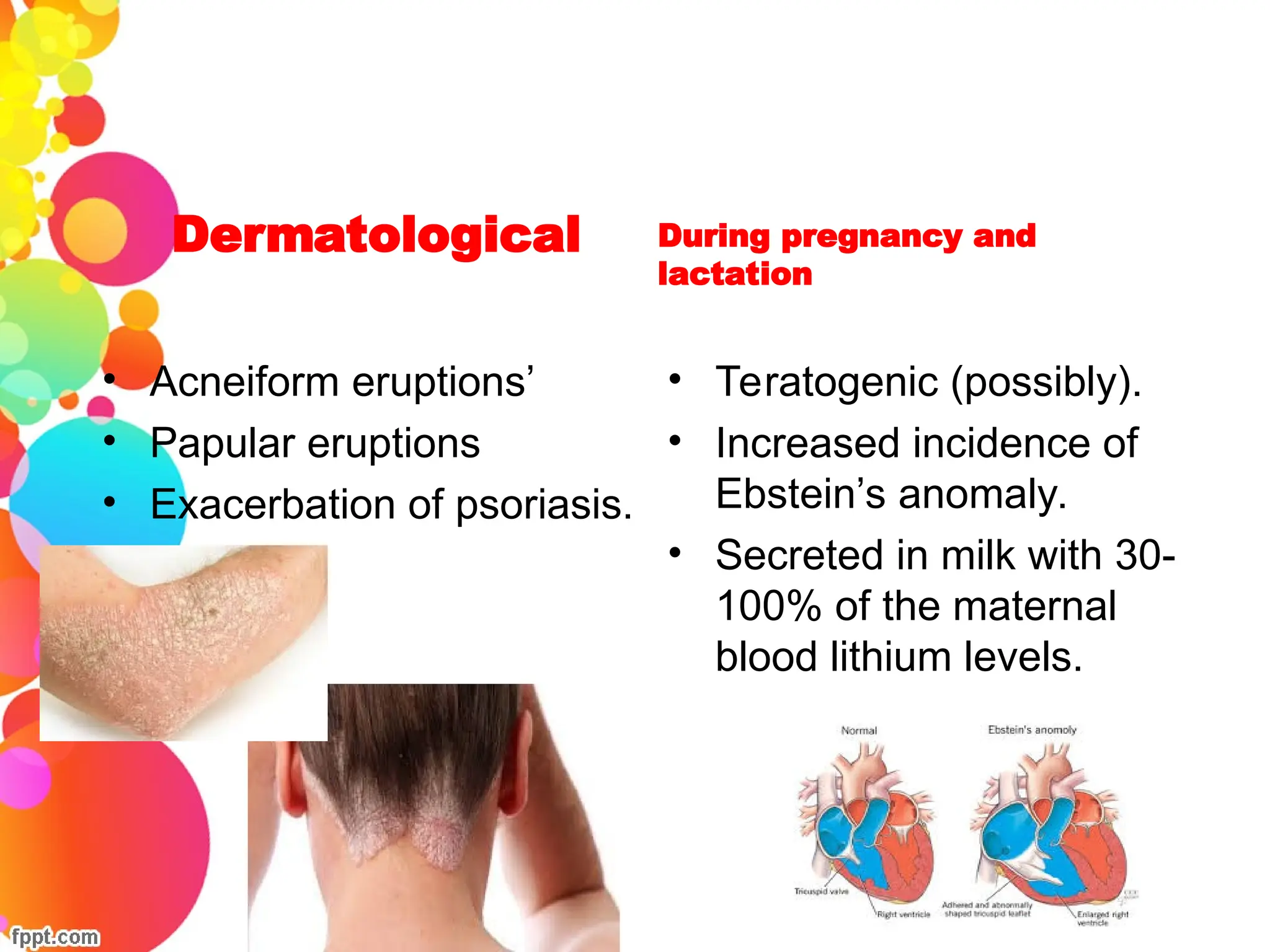
Dermatological
• Acneiform eruptions’
•Papular eruptions
• Exacerbation of psoriasis.
During pregnancy and
lactation
• Teratogenic (possibly).
• Increased incidence of
Ebstein’s anomaly.
• Secreted in milk with 30-
100% of the maternal
blood lithium levels.
23.
Management of lithiumtoxicity
• Discontinue the drug immediately.
• For significant short term indigestions,
residual gastric content should be removed
by induction of emesis, gastric lavage and
adsorption with activated charchol.
• If possible instruct the patient to ingest
fluids.
24.
Contd…
• Assess serumlithium levels, serum
electrolytes, renal functions, ECG as soon as
possible.
• Maintenance of fluid and electrolyte
imbalance.
• In a patient with serious manifestations of
lithium toxicity, hemodialysis should be
initiated.
25.
Nurse’s responsibilities fora
patient receiving Lithium
• The pre lithium work up:
• Routine general and systemic physical examination.
• Routine blood counts (Hb, TC, DC).
• Urine: routine and microscopic examination.
• ECG.
• Renal function tests
• Thyroid function tests
26.
Health advices tobe given
• Lithium must be taken on a regular basis, preferably at
the same time daily.
• When lithium therapy is initiated, mild side effects may
develop. Most of the are transient and do not represent
lithium toxicity.
• Serious side effects of lithium that necessitate its
discontinuance include vomiting, extreme hand tremors,
sedation, muscle weakness and vertigo. The psychiatrist
should be notified immediately if one of these effects
occur.
27.
Contd…
• Not todrive or operate dangerous machinery until lithium levels
are stabilized.
• Not skimp on dietery sodium intake. He or she should eat a
variety of health foods and avoid junk foods.
• The client should drink 6 to 8 large glasses of water each day
and avoid excessive use of beverages containing caffieine
(coffee, tea, colas), which promotes increased urine outfit.
• Carry card or other identification noting that he or she is taking
lithium.
28.
Contd…
• During treatmentit is essential to estimate blood
lithium levels at regular intervals (usually 3
monthly).
• The blood sample for estimation is taken 12 hours
after the last lithium dose.
• If any changes are made in lithium dosage, the
next blood level is estimated after at least 5-7 days
of the last change.
29.
Contd..
• The patientshould be told about the
importance of regular follow up. In every
six months, blood sample should be taken
for estimation of electrolytes, urea,
creatinine, a full blood count and thyroid
function test.
30.
To avoid teratogeniceffect
• Be aware of risks of becoming pregnant while
receiving lithium therapy.
• Use information furnished by health care providers
regarding methods of contraception.
• Notify the physician as soon as possible if
pregnancy is suspected or planned.
31.
Valproate
• Valproic acidwas first synthesized by Burton and used as
an organic solvent.
• In 1963, Meunier serendipitously discovered the
antiepileptic properties of valproic acid, while Lambert
reported in 1966 that valpromide (a valproic acid
analogue) might be effective as an antimanic.
• It was approved by the US FDA as an antiepileptic drug for
absence seizures in 1978 and for the treatment of acute
mania (and for migraine headache prophylaxis) in 1996.
32.
Mechanism of action
•By interfering with calcium channels and sodium
channels, valproate is thought both to enhance the
inhibitory actions of gamma aminobutyric acid (GABA)
and to reduce the excitatory actions of glutamate.
Indications
• Co-morbid substanceabuse or other psychiatric
disorders.
• Later age at onset and/or shorter duration of illness
• History of poor response to lithium
• Dysphoric mania, mixed affective episodes, or rapid
cycling
• Organic/complicated mania associated with seizure
disorder, history of head trauma, or EEG
abnormalities
• D-M-I (Depression-Mania-Well Interval) pattern of
illness, as opposed to the M-D-I pattern
Nurse’s Responsibilities
• Advisethe patient to take the drug immediately
after food to reduce GI irritation.
• Advise regular follow up and periodic examination
of blood count, hepatic function and thyroid
function.
• Refrain from discontinuing the drug abruptly,
physician will administer orders for tapering the
drug when therapy is to be discontinued.
38.
Contd…
• Report thefollowing symptoms to the physician
immediately: skin rash, unusual bleeding,
spontaneous bruising, sore throat, fever, malaise,
dark urine and yellow skin or eyes.
• Do not drive or operate dangerous machinery until
reaction to the medication has been established.
• Avoid consuming alcoholic beverages and non-
prescription medications without approval from
physician.
• Carry card at all times identifying the name of
medication being taken.
39.
Carbamazepine
• It isa tricyclic compound synthesized in 1953 by Schindler.
• Pharmacokinetics: The onset of action can be faster as
compared to lithium, but slower compared to valproate.
• Dosage: The usual dose is 600-1600 mg/day orally, in divided
doses. The treatment is best monitored with repeated blood
level. The therapeutic blood levels are 4-12 μg/ml and the
toxic blood levels are usually reached at >15 μg/ml.
•
40.
Mechanism of action
•By interfering with sodium and potassium,
carbamazepine is thought to enhance the inhibitory
actions of gamma aminobutyric acid (GABA).
Nurse’s responsibility
• Sincethe drug may cause dizziness and drowsiness
advise him to avoid driving and other activities requiring
alertness.
• Advise patient not to consume alcohol when it is on the
drug.
• Emphasize the importance of regular follow up visits and
periodic examination of blood count and monitoring of
cardiac renal, hepatic and bone marrow functions.
Conclusion
• Having groupedlithium, valproate and carmazepine
together, it is important to note they have subtle
differences in their therapeutic profiles and differential
predictors of response. Response to one of these
agents is not predictive of either a positive or negative
response to the others.