Downloaded 91 times
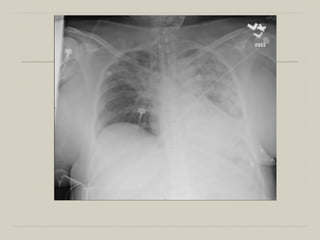



This patient likely has nosocomial pneumonia (either HAP or VAP) secondary to his multiple hospital admissions and prolonged intubation. He presents with fever, altered mental status, and respiratory distress - consistent with pneumonia. Given his multiple comorbidities and ESRD, he is high risk for poor outcomes. Broad spectrum antibiotics and further diagnostic workup are indicated.















































