Downloaded 112 times

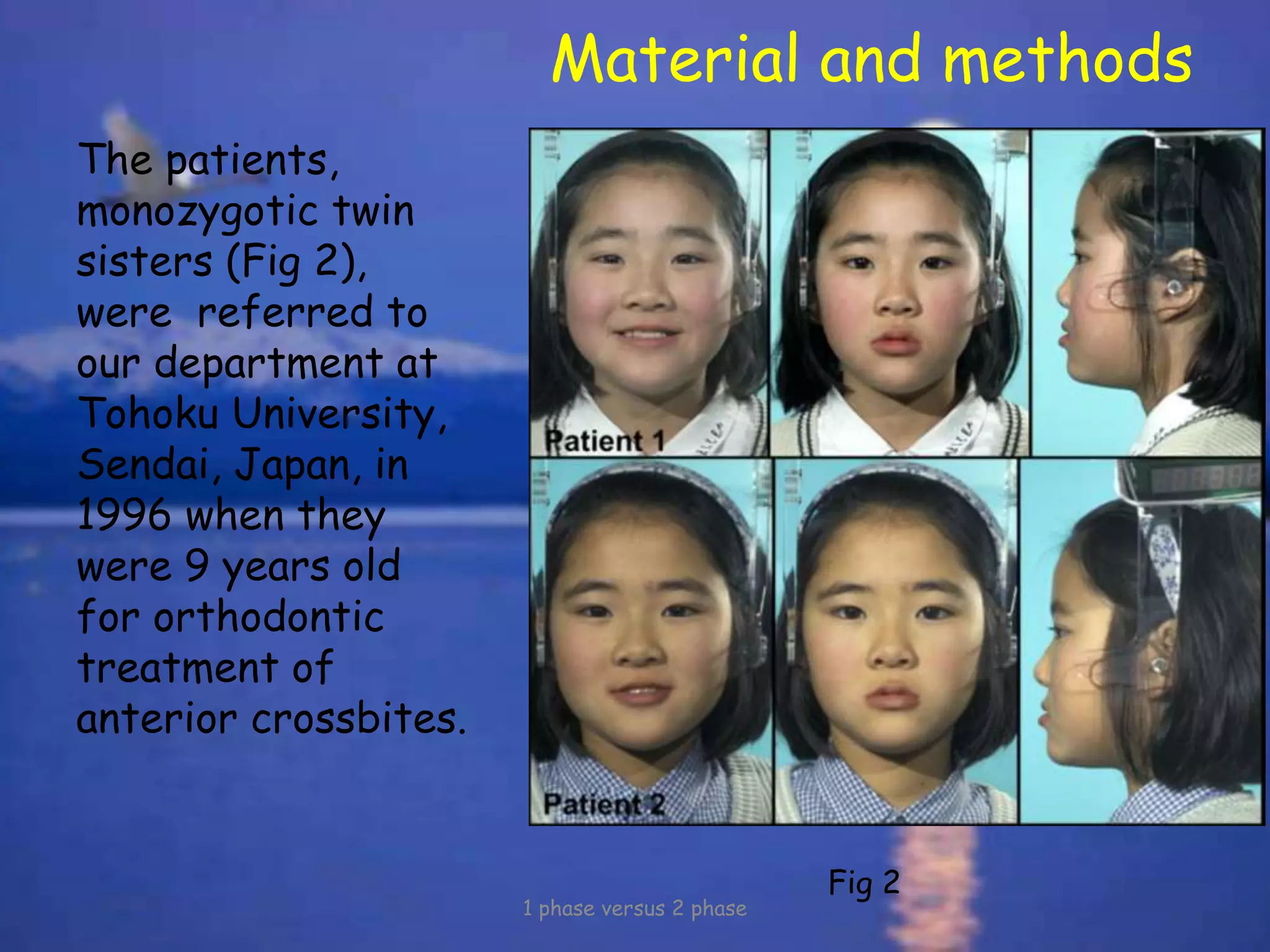
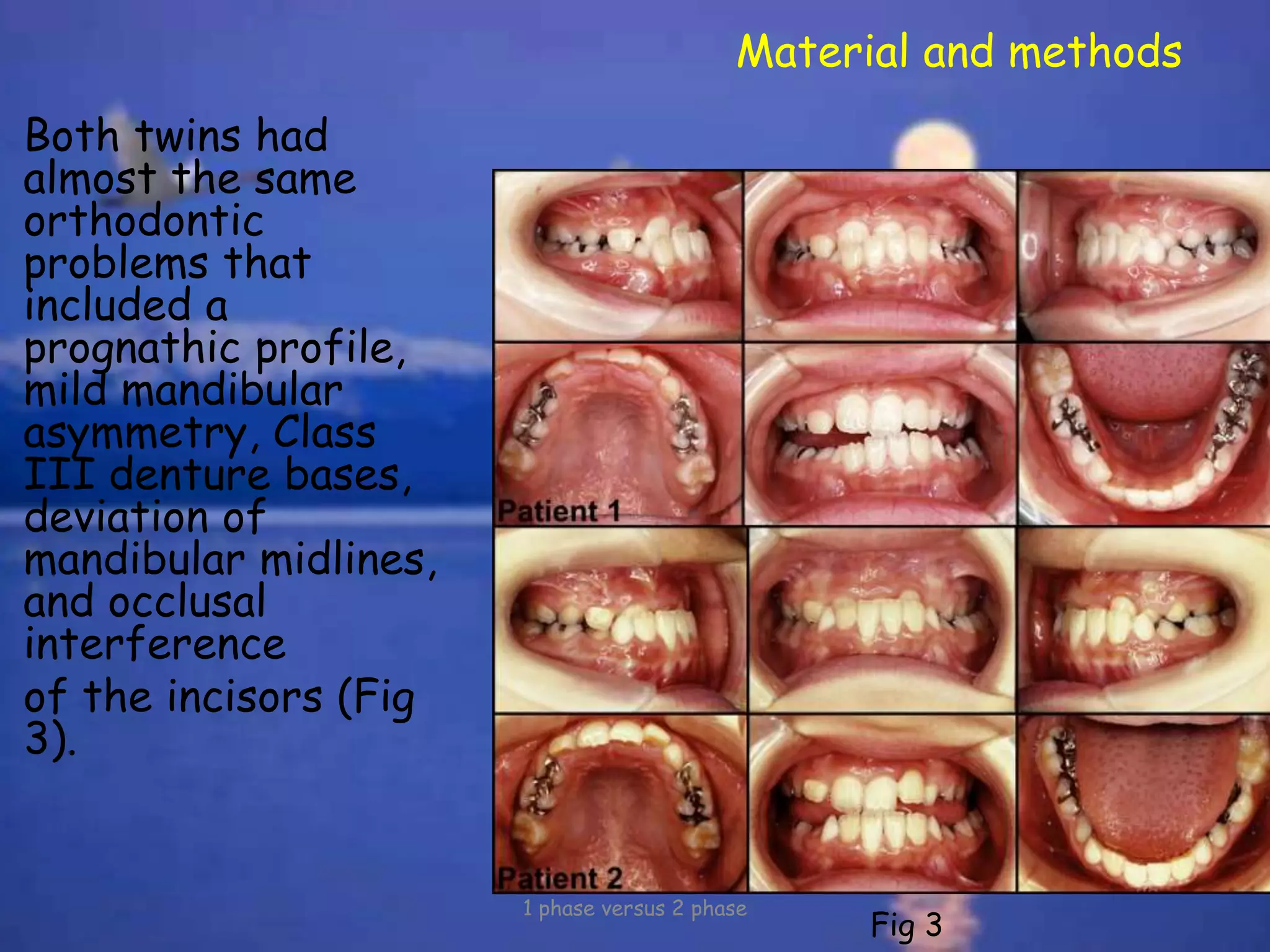
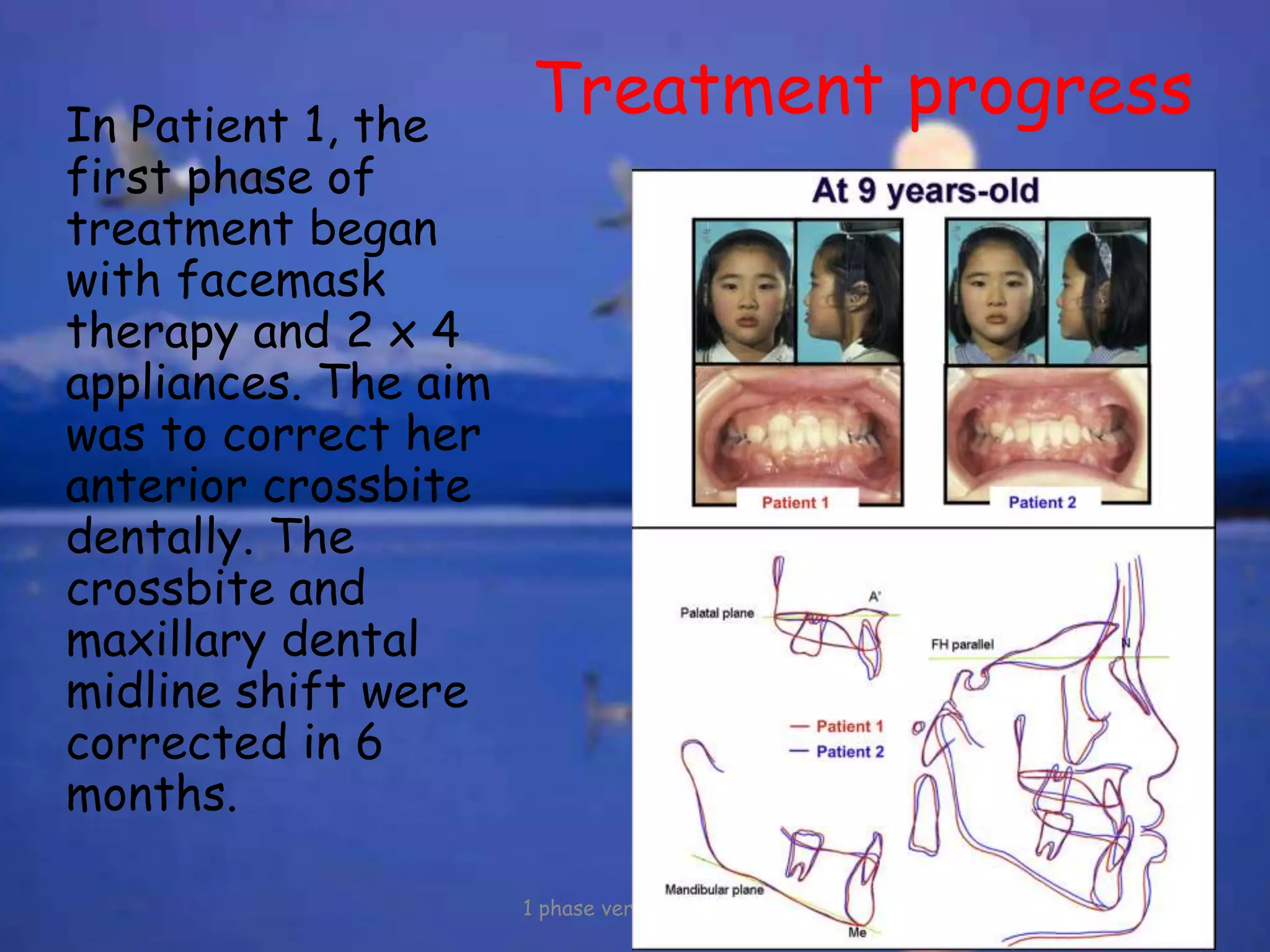
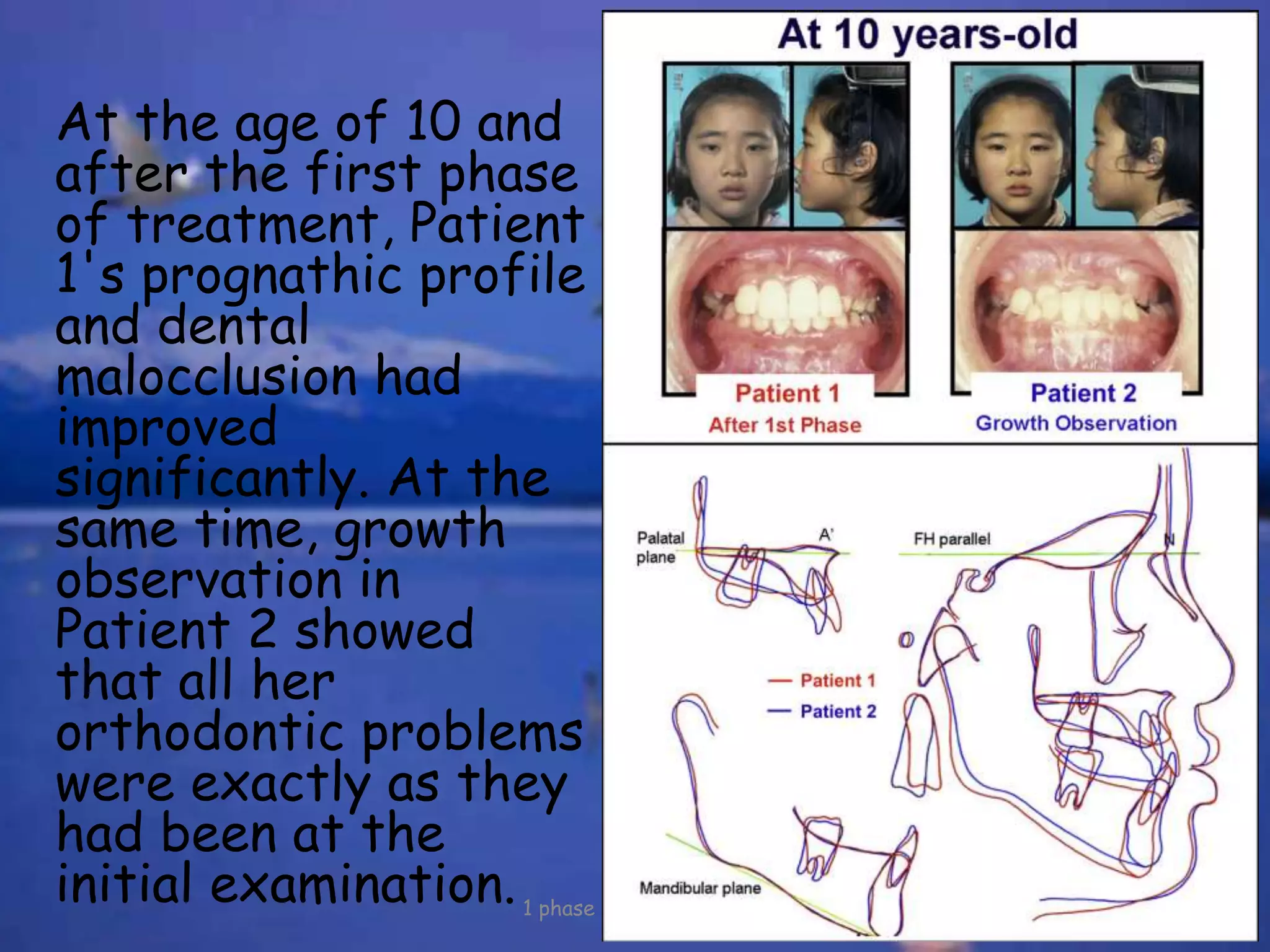
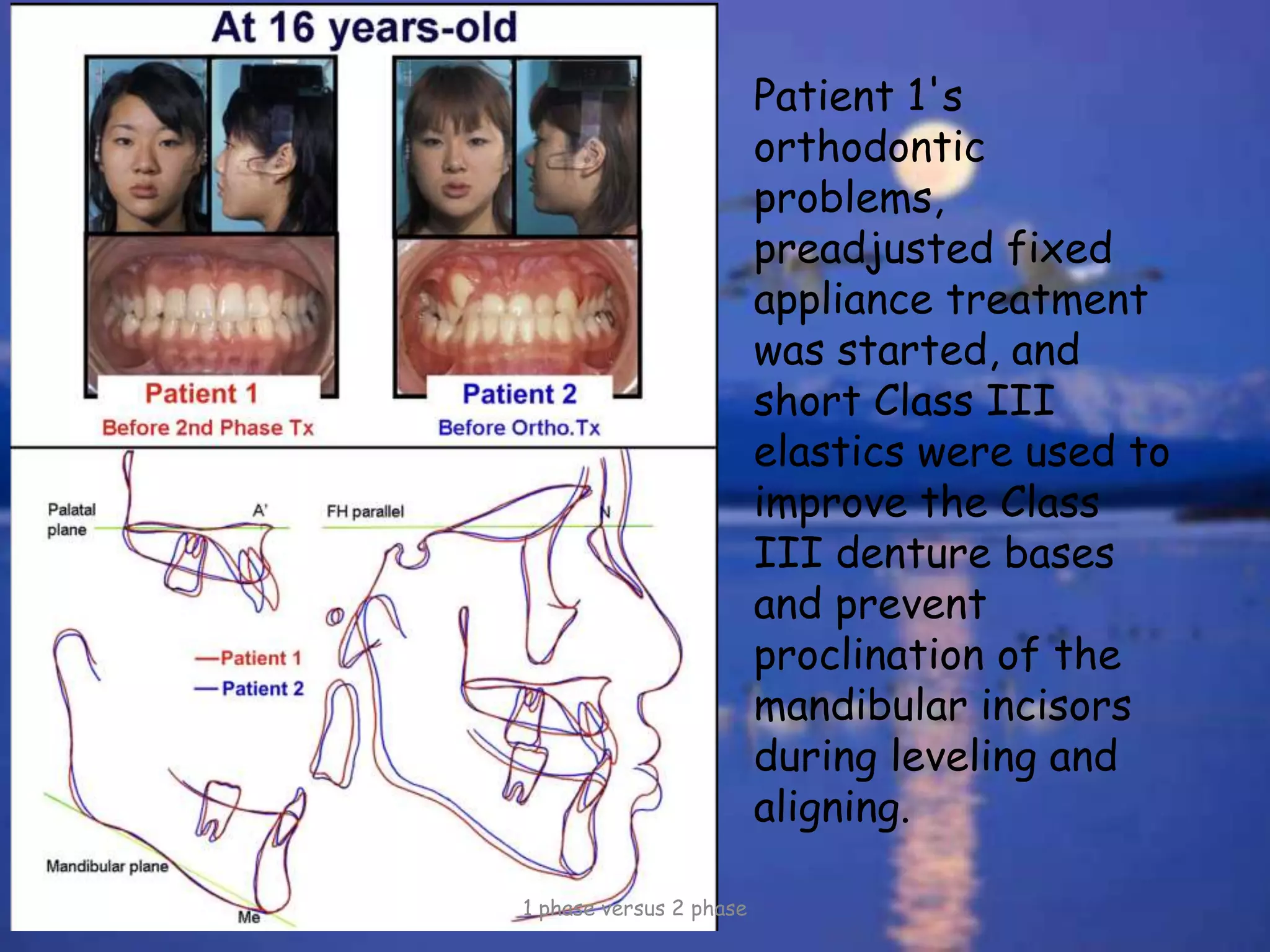
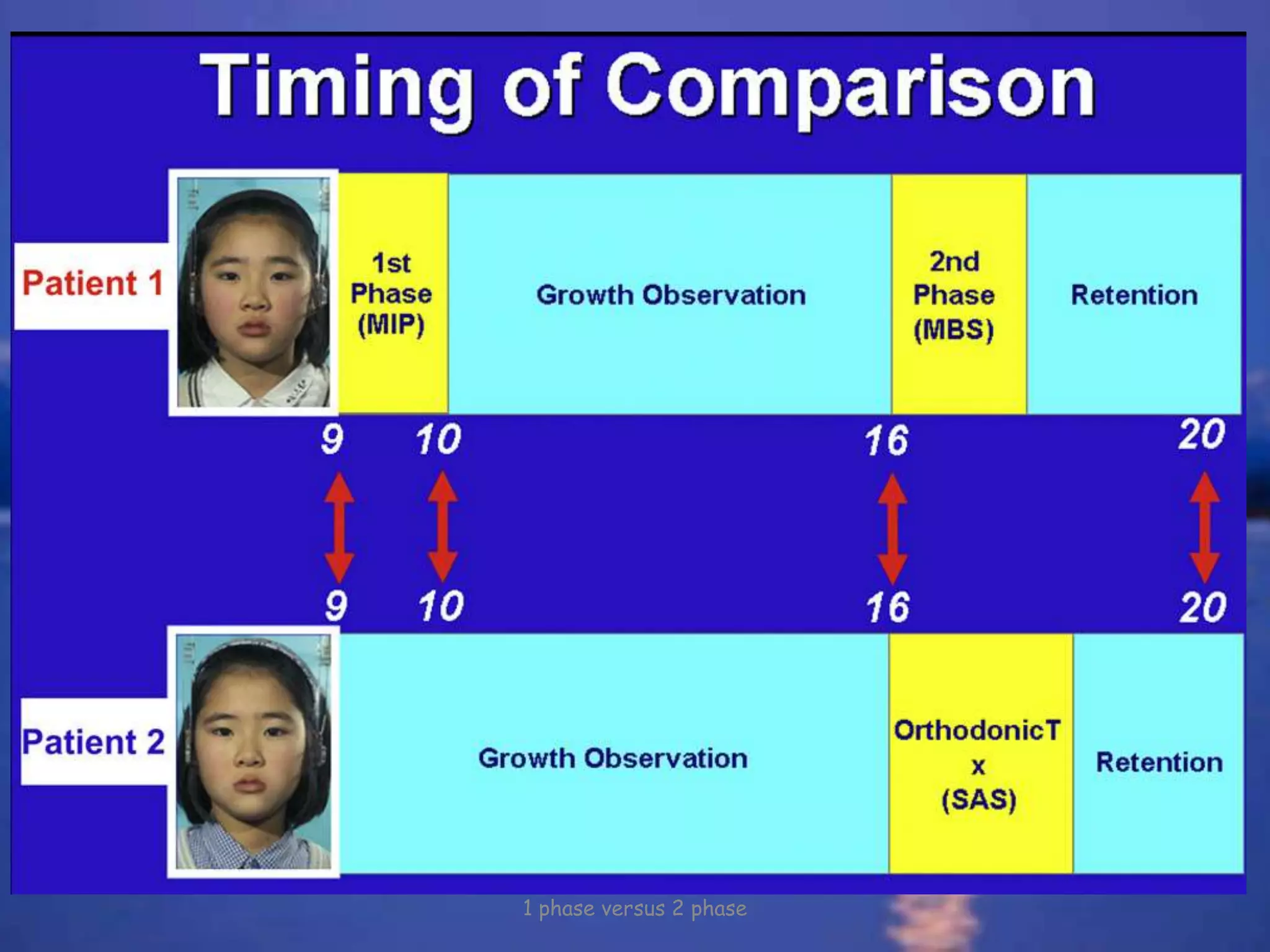

1. The study compared treatment outcomes for identical twin sisters with Class III malocclusions who underwent either 1-phase or 2-phase treatment. One twin received early crossbite correction followed by fixed appliances (2-phase), while the other received only fixed appliances (1-phase). 2. After treatment, both twins achieved almost identical dental results despite differences in treatment approach. This implied that early treatment had no impact on jaw growth, which was dominated by genetic factors. 3. While early treatment did not influence growth, it simplified subsequent treatment. Therefore, 2-phase treatment may be better suited than 1-phase treatment for mild-moderate Class III cases. However, criteria for the treatment approach depend on
































































































