Download as PDF, PPTX


![Editorial
Interscalene catheters - should we give them the cold shoulder?
The benefits of single-shot inter-
scalene brachial plexus blockade
(SSIB) for patients undergoing
shoulder surgery are well estab-
lished [1]. These blocks have a
consistently high success rate, the
techniques are well described [2–4]
and are suitable for the vast major-
ity of patients presenting for
shoulder surgery. Single-shot blocks
can provide excellent analgesia for
11-14 hours, which mitigates the
severe postoperative pain that can
follow shoulder surgery. In the
UK, these patients are commonly
that, at the moment, ambulatory
catheter techniques for shoulder
surgery are not widely employed,
and this may be related to logistical
and safety concerns. This seems to
be confirmed by the fact that there
are few published research papers
that have included more than
twenty patients [9]. Fredrickson
et al. should therefore be com-
mended for completing the largest
prospective observational study so
far that has investigated the safety
of such an analgesic regimen.
In approximately 1500 patients
dyspnoea during the infusion at
home, which was surprisingly high
at 27% and was in contrast to the
0.7% of patients who experienced
this symptom immediately postoper-
atively.
As anaesthetists, we are inter-
ested in pain and dyspnoea, but
patients often have different con-
cerns, and they may find numbness
just as unpleasant as pain, thus
influencing their choice of analgesic
technique. It would have been inter-
esting to learn how patients per-
ceived their recovery with
Anaesthesia 2016, 71, 359–372
houlder surgery
llow same day
ajority of cases.
eliable analgesia
ich can be pro-
se of adjuncts
ic receptor ago-
hasone, but the
of these drugs
ptake [20]. Sig-
article reported
of analgesia of
th a single dose
methasone com-
ral dexametha-
evelopment of
mulations such
caine may offer
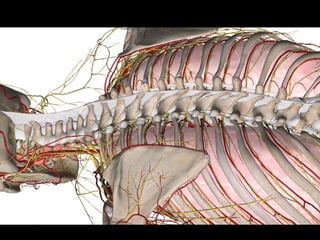
before the branching of the supras-
capular nerve [25]. Performing a
nerve block at this level can provide
adequate analgesia for shoulder sur-
gery and may be less likely to result
in phrenic nerve palsy. Although
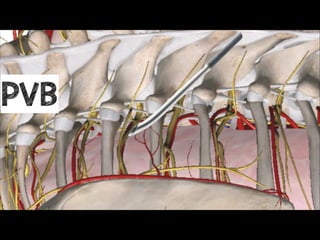
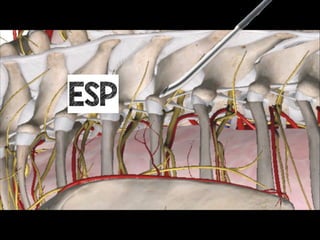
not commonly performed, the supe-
rior trunk block could provide a
safer target for catheter placement
because the locations of the needle
and catheter tip should be easily
visible when using ultrasound. A
recent letter by Lin et al. described
a single puncture approach to block
both the supraclavicular nerves and
the superior trunk of the brachial
plexus [26], however much more
work is required to determine the
up the level of knowledge and skill
in the wider anaesthesia community
to allow us to offer this service
safely.
Acknowledgements
No external funding and no com-
peting interests declared.
A. Pawa
Consultant
A. P. Devlin
A. Kochhar
Specialty Registrars
Department of Anaesthesia
Guy’s and St. Thomas’ Hospitals
London UK
Email: amit.pawa@gstt.nhs.uk
naesthetists of Great Britain and Ireland 361
@amit_pawa](https://image.slidesharecdn.com/peripheralnervecathteters-191208175820/85/Peripheral-Nerve-Catheters-an-introduction-5-320.jpg)

























Dr. Amit Pawa discusses the use of peripheral nerve catheters for analgesia in shoulder surgery, highlighting the effectiveness of single-shot interscalene blocks and the potential benefits of catheter techniques despite current logistical challenges. The document emphasizes the importance of patient selection, safety during catheter placement, and multimodal analgesia to improve postoperative outcomes. It also reviews complications and suggests improvements for catheter use based on a retrospective study conducted at Guy's Hospital.
















































































