

![5521 Ruffin Road
San Diego, CA 92123
e-mail: information@pluralpublishing.com
Website: https://www.pluralpublishing.com
Copyright © 2020 by Plural Publishing, Inc.
Typeset in 10.5/13 Minion Pro by Flanagan’s Publishing Services, Inc.
Printed in the United States of America by McNaughton & Gunn, Inc.
All rights, including that of translation, reserved. No part of this publication may be
reproduced, stored in a retrieval system, or transmitted in any form or by any means,
electronic, mechanical, recording, or otherwise, including photocopying, recording, taping,
Web distribution, or information storage and retrieval systems without the prior written
consent of the publisher.
For permission to use material from this text, contact us by
Telephone: (866) 758-7251
Fax: (888) 758-7255
e-mail: permissions@pluralpublishing.com
Every attempt has been made to contact the copyright holders for material originally printed in
another source. If any have been inadvertently overlooked, the publishers will gladly make the
necessary arrangements at the first opportunity.
Library of Congress Cataloging-in-Publication Data
Names: Arvedson, Joan C., author, editor. | Brodsky, Linda, editor. |
Lefton-Greif, Maureen A., author, editor.
Title: Pediatric swallowing and feeding : assessment and management / Joan C.
Arvedson, Linda Brodsky, Maureen A. Lefton-Greif.
Description: Third edition. | San Diego, CA : Plural Publishing, [2020] |
Includes bibliographical references and index.
Identifiers: LCCN 2019013064| ISBN 9781944883515 (alk. paper) | ISBN
1944883517 (alk. paper)
Subjects: | MESH: Feeding and Eating Disorders of Childhood | Deglutition
Disorders | Feeding Behavior—physiology | Deglutition—physiology |
Infant | Child
Classification: LCC RJ463.I54 | NLM WM 175 | DDC 618.92/31—dc23
LC record available at https://lccn.loc.gov/2019013064
Disclaimer: Please note that ancillary content (such as documents, audio, and video,
etc.) may not be included as published in the original print version of this book.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-5-320.jpg)













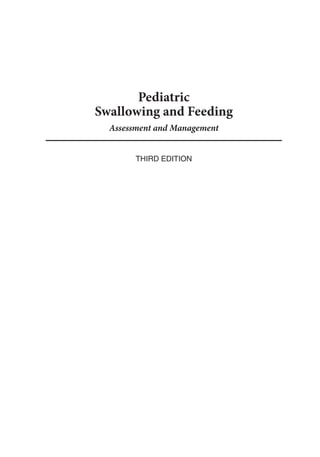
![2 Pediatric Swallowing and Feeding: Assessment and Management
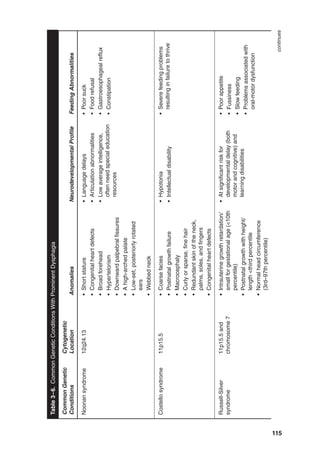
Prevalence
Currently, more than 100,000 newborn
infants are given diagnoses of feeding prob-
lems after being discharged from acute care
hospitals, and more than one-half mil-
lion children (3–17 years) in the United
States are diagnosed with dysphagia annu-
ally (Bhattacharyya, 2015; CDC/NCHS
National Hospital Discharge Survey, 2010).
The number of children with swallowing
and feeding disorders has been increasing
in part due to recent medical and techno-
logical advances, which have improved the
survival of many infants and children who
previously would not have survived. The
range and complexity of their problems
will continue to challenge the health care,
educational, and habilitation/rehabilitation
systems because many of these children are
now living longer, remaining healthier, and
having greater expectations for leading full
and productive lives.
Approximately 40% of children born
preterm have swallowing/feeding disorders.
Globally, an estimated 15 million infants are
born preterm (less than 37 weeks’ gestation),
and the number is increasing (World Health
Organization [WHO], 2017). Although
many children and their families have ben-
efited greatly, the increasing number of chil-
dren born prematurely at low birth weight
(less than 2,500 g), very low birth weight (less
than 1,500 g), and extremely low birth weight
(less than 600 g) are frequently confronted
with multiple complex medical problems.
In comparison to full-term infants, late
preterm infants (34-0/7 to 36-6/7 weeks
gestation) are at increased risk for respira-
tory and neurologic complications that may
produce or exacerbate feeding difficulties
(Engle, Tomashek, & Wallman, 2007; Mally,
Bailey, & Hendricks-Munoz, 2010). Other
infants with genetic, cardiac, and gastroin-
testinal abnormalities are faced with com-
plex medical and in some instances surgical
problems. Early recognition and interven-
tion have been invaluable despite the cog-
nitive disabilities, cerebral palsy, chronic
pulmonary problems, structural deficits,
and neurologic impairments that infants
endure. Swallowing and feeding problems
compound most of these conditions.
Developmental
Considerations
After the establishment of adequate respi-
ration and physiologic stability, the highest
priority for caregivers is to meet the nutri-
tional needs of their newborn infants. To
achieve this goal successfully, infants and
children of all ages require a well-func-
tioning oral sensorimotor and swallow-
ing mechanism, overall adequate health
(including respiratory, gastrointestinal, and
neurologic), appropriate nutrition, central
nervous system integration, and adequate
musculoskeletal tone.
In addition, the emergence of commu-
nication, an often-overlooked process, is
closely aligned with successful swallowing
and feeding, particularly in young children
(Malas, Trudeau, Chagnon, & McFarland,
2015). Normal feeding patterns are reflected
in the early developmental pathways that
sequentially and rapidly emerge during the
first several months and years of life. Com-
munication is one of the most important
of those pathways. The interrelationship
between feeding, shared by all biologic crea-
tures, and language-based, verbal commu-
nication, unique to humans, cannot be over-
emphasized. The comparative anatomy of
the upper aerodigestive tract and its impli-](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-19-320.jpg)




























































![2. Anatomy, Embryology, Physiology, and Normal Development 65
Amaizu, N., Shulman, R., Schanler, R., Lau,
C. (2008). Maturation of oral feeding skills
in preterm infants. Acta Paediatrica, 97(1),
61–67. doi:10.1111/j.1651-2227.2007.00548.x
American Academy of Pediatrics. (2012). Breast-
feeding and the use of human milk. Pedi-
atrics, 129(3), e827–e841. Retrieved from
http://pediatrics.aappublications.org/con
tent/129/3/e827.full.pdf+html
Anderson, V., Spencer-Smith, M., Wood, A.
(2011). Do children really recover better?
Neurobehavioural plasticity after early brain
insult. Brain, 134(Pt 8), 2197–2221. doi:10.10
93/brain/awr103
Ardran, G., Kemp F. (1952). The protection of
the laryngeal airway during swallowing. Brit-
ish Journal of Radiology, 25, 406–416.
Ardran, G., Kemp F. (1956). Closure and
opening of the larynx during swallowing.
British Journal of Radiology, 29, 205–208.
Arvedson, J., Lefton-Greif, M. A. (1998).
Pediatric videofluoroscopic swallow studies:
A professional manual with caregiver guide-
lines. San Antonio, TX: Communication Skill
Builders.
Barclay, A. E. (1930). The normal mechanism
of swallowing. British Journal of Radiology,
3, 534–546.
Barker, G. R., Cochrans, G. M., Corbett, G. A.,
Hunt, J. N. (1974). Actions of glucose and
potassium chloride osmoreceptors slowing
gastric emptying. Journal of Physiology, 237,
183–186.
Beauchamp, G. K., Mennella, J. A. (1998). Sen-
sitive periods in the development of human
flavor perception and preference. In Annales
Nestle, Nestle Nutrition Workshop Series, 56,
19–31. Vevey, Switzerland: Nestec.
Berg, K. L. (1990). Tongue-tie (ankyloglos-
sia) and breastfeeding: A review. Journal of
Human Lactation, 6, 109–112.
Bloomfield, F. H., Harding, J. E., Meyer, M. P.,
Alsweiler, J. M., Jiang, Y., Wall, C. R., Alexan-
der, T., DIAMOND Study Group. (2018).
The DIAMOND trial—Different approaches
to moderate and late preterm nutrition:
Determinants of feed tolerance, body com-
position and development: Protocol of a
randomised trial. BMC Pediatrics, 18(1), 220.
doi:10.1186/s12887-018-1195-7
Boeck, A., Buckley, R. H., Schiff, R. I. (1997).
Gastroesophageal reflux and severe com-
bined immunodeficiency. Journal of Allergy
Clinics Immunology, 99, 420–424.
Boix-Ochoa, L., Canals, J. (1976). Maturation
of the lower esophagus. Journal of Pediatric
Surgery, 11, 749–756.
Bosma, J. F. (1967). Human infant oral function.
In J. F. Bosma (Ed.), Oral sensation and per-
ception (pp. 98–110). Springfield, IL: Charles
C. Thomas.
Bosma, J. F. (1972). Form and function in the
infant’s mouth and pharynx. In J. F. Bosma
(Ed.), Oral sensation and perception: The
mouth of the infant (pp. 3–19). Springfield,
IL: Charles C. Thomas.
Bosma, J. F. (1986). Development of feeding.
Clinical Nutrition, 5, 210–218.
Bosma, J. F. (1988). Functional anatomy of the
upper airway during development. In O. P.
Mathew G. Sant’Ambrogio (Eds.), Respira-
tory function of the upper airway (pp. 47–86).
New York, NY: Marcel Dekker.
Brazelton, T. B. (1969). Infants and mothers. New
York, NY: Dell.
Brookes, M., Zietman, A. (1998). Clinical em-
bryology: A color atlas and text. Boca Raton,
FL: CRC Press.
Brown, H. K., Speechley, K. N., Macnab, J.,
Natale, R., Campbell, M. K. (2014). Neo-
natal morbidity associated with late preterm
and early term birth: The roles of gestational
age and biological determinants of preterm
birth. International Journal of Epidemiology,
43, 802–814.
Burdi, A. R. (1969). Sexual differences in clo-
sure of the human palatal shelves. Cleft Palate
Journal, 6, 1–4.
Burke, P. M. (1977). Swallowing and the orga-
nization of sucking in the human newborn.
Child Development, 48, 523–531.
Cagan, J. (1995). Feeding readiness behavior in
preterm infants [Abstract]. Neonatal Net-
work, 14, 82.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-82-320.jpg)





![2. Anatomy, Embryology, Physiology, and Normal Development 71
trolled trial of parental counseling. Pediatrics,
106, 483–488.
Nishino, T. (2013). The swallowing reflex and
its significance as an airway defensive reflex.
Frontiers in Physiology, 3, Article 489.
Perkin, M. R., Bahnson, H. T., Logan, K., Marrs,
T., Radulovic, S., Craven, J., . . . Lack, G.
(2018). Association of early introduction of
solids with infant sleep: A secondary analysis
of a randomized clinical trial. JAMA Pediat-
rics, 172(8), e180739. doi:10.1001/jama
pedi
atrics.2018.0739
Perlman, A. L., Christensen, J. (1997). Topog-
raphy and functional anatomy of the swal-
lowing structures. In A. L. Perlman K. S.
Schulze-Delrieu (Eds.), Deglutition and its
disorders: Anatomy, physiology, clinical diag-
nosis, and management (pp. 15–42). San
Diego, CA: Singular.
Perlman, A. L., Schulze-Delrieu, K. S. (Eds.).
(1997). Deglutition and its disorders: Anat-
omy, physiology, clinical diagnosis, and man-
agement. San Diego, CA: Singular.
Persaud, T. V. N., Chudley, A. E., Skalko, R.
F. (1985). Basic concepts in teratology. New
York, NY: Alan R. Liss.
Perugu, S. (2010). Late preterm births: Epide-
miology, possible causes, and consequences.
Journal of Neonatal-Perinatal Medicine, 3(4),
259–269.
Petrosyan, M., Shah, A. A., Chahine, A. A., Guz
zetta, P. C., Sandler, A. D., Kane, T. D. (2018).
Congenital paraesophageal hernia: Contem-
porary results and outcomes of laparoscopic
approach to repair in symptomatic infants
and children. Journal of Pediatric Surgery.
doi:10.1016/j.jpedsurg.2018.07.008
Prades, J. M., Timoshenko, A. P., Asanau, A.,
Gavid, M., Benakki, H., Dubois, M. D., . . .
Martin, C. (2009). The cricopharyngeal mus-
cle and the laryngeal nerves: Contribution to
the functional anatomy of swallowing. [Arti-
cle in French]. Morphologie, 93(301), 35–41.
doi:10.1016/j.morpho.2009.07.001
Praud, J. P. (2010). Upper airway reflexes in
response to gastric reflux. Pediatric Respira-
tory Reviews, 11(4), 208–212.
Pridham, K. F. (1990). Feeding behavior of 6–12
month old infants: Assessment of sources
of parental information. Journal of Pediatric
Nursing, 117, S174–S180
Pridham, K. F., Martin, R., Sondel, S., Tluczek,
A. (1989). Parental issues in feeding young
children with bronchopulmonary dysplasia.
Journal of Pediatric Nursing, 4, 177–185.
Rogers, B., Arvedson, J., Msall, M., Demerath,
R. (1993). Hypoxemia during oral feeding of
children with severe cerebral palsy. Devel-
opmental Medicine and Child Neurology, 35,
3–10.
Roman, C. (1966). Nervous control of esopha-
geal peristalsis. Journal De Physiologie, 58,
79–108.
Roman, C., Tieffenbach, L. (1972). Record-
ing the unit activity of vagal motor fibers
innervating the baboon esophagus. Journal
De Physiologie, 64, 479–506.
Rosano, A., Smithells, D., Cacciani, L., Botting,
B., Castilla, E., Cornel, M., . . . Sumiyoshi, Y.
(1999). Time trends in neural tube defects
prevalence in relation to preventive strate-
gies: An international study. Journal of Epide-
miology and Community Health, 53, 630–635.
Rosen, C. L., Glaze, D. G., Frost, J. D. Jr.
(1984). Hypoxemia associated with feeding
in the preterm infant and full-term neonate.
American Journal Diseases Children, 138,
623–628.
Sahni, R., Polin, R. A. (2013). Physiologic
underpinnings for clinical problems in mod-
erately preterm and late preterm infants.
Clinical Perinatology, 40, 645–663.
Saitoh, E., Shibata, S., Matsuo, K., Baba, M., Fujii,
W., Palmer, J. B. (2007). Chewing and food
consistency: Effects on bolus transport and
swallow initiation. Dysphagia, 22(2), 100–
107. doi:10.1007/s00455-006-9060-5
Sakalidis, V. S., Geddes, D. T. (2016). Suck-
swallow-breathe dynamics in breastfed in-
fants. Journal of Human Lactation, 32(2),
210–211.
Sasaki, C. T. (2000). Understanding the motor
innervation of the human cricopharyn-
geus muscle. American Journal of Medicine,
108(Suppl. 4a), 38S–39S.
Sasaki, C. T., Isaacson, G. (1988). Functional
anatomy of the larynx. Otolaryngology Clinics
of North America, 21, 196–199.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-88-320.jpg)











![84 Pediatric Swallowing and Feeding: Assessment and Management
in infancy with the majority having difficul-
ties related to the tongue or jaw (e.g., chew-
ing or swallowing) (Robinson, 1990).
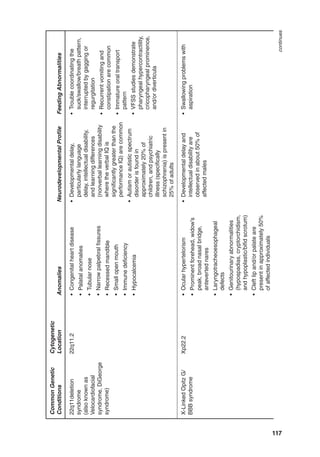
A variety of medications may influence
neurologic function, including motor devel-
opment, cognition, and feeding abilities.
A basic understanding of brain stem neu-
rotransmitter systems is helpful in under-
standing the impact of medications on swal-
lowing. Glutamate, excitatory amino acids
(NMDA [N-methyl-D-aspartate receptor]
agonists)andmonoamines(dopamine)stim-
ulate, and catecholamines (clonidine) have
been shown to inhibit swallowing in various
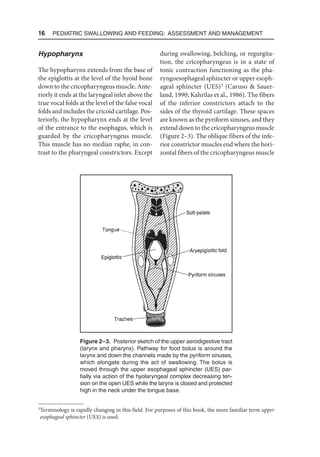
animal models (Jean, 2001). Table 3–1 lists
some medications and their actions on both
the central and peripheral nervous systems.
Commonly used anticonvulsants (including
carbamazepine, gabapentin, phenobarbital,
phenytoin, and valproic acid) and muscle
relaxants, including baclofen and cycloben-
zaprine, may produce drowsiness (Balzer,
2000). Benzodiazepines are used as anti-
convulsants and occasionally for treatment
of spasticity. In addition to their sedative
effects, benzodiazepines may directly reduce
activity in brain stem centers that regulate
swallowing (Buchholz, 1995; Wyllie, Wyllie,
Cruse, Rothner, Ehrenberg, 1986). Dopa-
mine antagonists, including the neurolep-
tics, are often used for agitation and aggres-
sive behavior in children with cognitive and
communicative impairments. These medi-
cations have been associated with the devel-
opment of laryngeopharyngeal dystonia
and esophageal dysmotility (Moss Green,
1982; Sokoloff Pavlakovic, 1997; Sico
Patwa, 2011). Selective serotonin reuptake
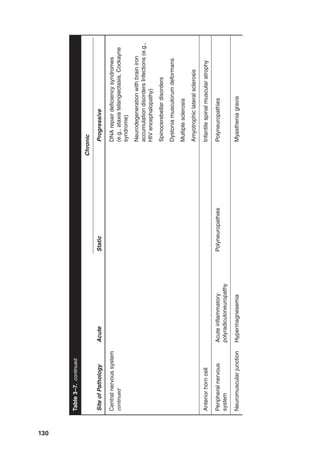
Table 3–1. Medication-Induced Nervous System Abnormalities Related to Dysphagia
Nervous System Abnormalities Medications
Central nervous system
Arousal Benzodiazepines
Chloral hydrate
Hydroxyzine
Antihistamines
Neuroleptics
Anticonvulsants (barbiturates, valproate,
carbamazepine, gabapentin, phenytoin)
Suppression of brain stem regulation Benzodiazepines
Movement disorders (e.g., tardive dyskinesia) Dopamine antagonists (e.g., neuroleptics)
Muscle relaxation Baclofen
Peripheral nervous system
Neuromuscular junction blockade Aminoglycosides
Myopathy Corticosteroids
Diminished salivation Anticholinergics (e.g., tricyclic
antidepressants and antihistamines)
Source: Adapted from Arvedson, J. C., Rogers, B. T. (Eds.). (1997). Pediatric dysphagia: Management
challenges for school-based speech language pathologist. Pittsburgh, PA: Rehabilitation Training Network
Health Care Group. Copyright 1997.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-101-320.jpg)





















































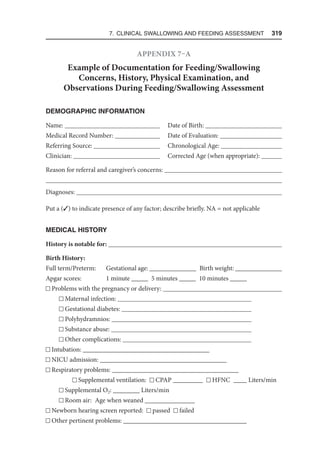
![154 Pediatric Swallowing and Feeding: Assessment and Management
well as during feeding. The presence of overt
airway obstruction should prompt imme-
diate examination of the airway. Signs of
airway distress are often absent until feeds
are introduced and may include snorting,
grunting, head bobbing, an increased rate of
breathing (tachypnea) and frequent pauses
between swallows that may indicate a con-
comitant airway problem.
When oral feeding is associated with
significant airway distress, such as severe
coughing, cyanosis, apnea, bradycardia or
choking, it may need to be discontinued
until the etiology is determined, the prob-
lem resolves (e.g., infection, obstruction), or
the airway distress is stabilized, and swal-
lowing may be assessed. The triad of chok-
ing, coughing, and cyanosis that occurs
with oral feeding is most commonly seen
in unrecognized tracheoesophageal fistula
(TEF) or laryngeal cleft, particularly in an
infant who has had recurrent pneumonia
during the first few months of life. When a
high-pitched stridor in infants coexists with
coughing, choking, and cyanosis, laryngo-
malacia should be considered as well.
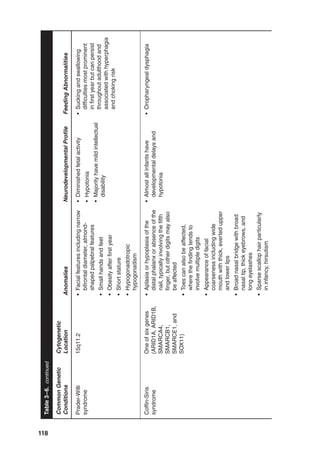
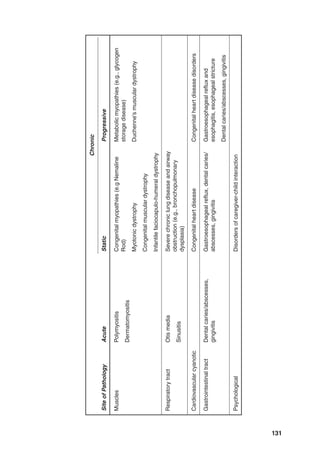
Craniofacial findings may include man-
dibular hypoplasia (Figure 4–1) or asym-
metry seen in hemifacial microsomia,
indicating abnormal soft tissue structures
or tongue position that may interfere with
feeding. Feeding difficulties can occur
with various degrees of palatal clefting see
(Chapter 12). Identification of a submucous
cleft palate (Figure 4–2) requires intraoral
examination for bifid uvula, a zona pellu-
cida (submucosal absence of the muscula-
ris uvulae), and notching of the hard palate.
Figure 4–1. A. Infant with micrognathic mandible from an isolated Pierre Robin
sequence. B. U-shaped cleft palate also characteristic of Pierre Robin sequence.
(Source: From Volk, M. S., Arnold, S., Brodsky, L. [1992]. Otolaryngology and
audiology. In L. Brodsky, L. Holt, D. H. Ritter-Schmidt (Eds.), Craniofacial
anomalies: An interdisciplinary approach [p. 169]. St. Louis, MO: Mosby-Year
Book. Copyright 1992 by Mosby-Year Book. Reprinted by permission.)
A B](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-171-320.jpg)





![160 Pediatric Swallowing and Feeding: Assessment and Management
Retardation, Genitourinary, and Ear abnor-
malities). Children with CHARGE syn-
drome almost always have neurodevelop-
mental delays associated with decreased
neuromuscular tone and incoordination, all
further complicating feeding. Tracheostomy
offers the most effective means for managing
the airway in some of these children (Asher,
McGill, Kaplan, Friedman, Healy, 1990).
Others may require long-term gastrostomy
tube feeding supplements (Dobbelsteyn,
Peacocke, Blake, Crist, Rashid, 2008).
Inspection of both posterior nasal cho-
anae using FFNL with a 2-mm or 3-mm
endoscope or a 2.7-mm rigid telescope is
most helpful. Direct visualization, combined
with axial computed tomographic scan of
the nose and nasopharynx, will determine
the type (membranous versus bony) and
the extent of the lesion (Figure 4–5). Sur-
gical repair of bilateral choanal atresia is
usually performed in the neonatal period
(Figure 4–6). The transnasal approach is
preferred in this age group by most (Eladl
Khafagy, 2016; Gulşen et al., 2017; Lantz
Birck, 1981; Richardson Osguthorpe,
1988). Transnasal approach with short-term
stenting was not found to decrease the inci-
dence of reclosure and restenosis of the pos-
terior choanae, but did have higher compli-
Figure 4–5. Axial computed tomographic scan
showing bilateral bony choanal atresia. (Source:
From Volk, M. S., Arnold, S., Brodsky, L. Otolar-
yngology and audiology. In L. Brodsky, L. Holt, D.
H. Ritter-Schmidt [Eds.], Craniofacial anomalies: An
interdisciplinary approach [p. 172]. St. Louis, MO:
Mosby-Year Book. Copyright 1992 by Mosby-Year
Book. Reprinted by permission.)](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-177-320.jpg)


![4. The Upper Airway and Swallowing 163
way. Surgical treatment may occur soon
after diagnosis (or later for some). Surgi-
cal methods include open calvarial recon-
struction, minimally invasive strip craniec-
tomy with postoperative molding helmet,
minimally invasive strip craniectomy with
spring implantation, and cranial distrac-
tion (Governale, 2015). Müller-Hagedorn
and colleagues (2018) reported treatment
of airway obstruction with a modified Tub-
ingen Palatal Plate (TPP) as mostly effective
and safe. They emphasized the need for pro-
spective studies that may help avoid more
invasive procedures, such as tracheostomy,
for some children until the diameter of the
airway increases with growth. The airway
may be improved with midface advance-
ment, a procedure that has been performed
in some cases as early as age 3 years, but is
best deferred until after puberty.
Mandibular Hypoplasias
The Pierre Robin sequence classically has
been described by a triad of clinical signs
to include mandibular hypoplasia, micro-
gnathia, glossoptosis (backward, downward
placement of the tongue) (Figure 4–10), and
a U-shaped cleft palate (see Figure 4–1).
This condition is now labeled Pierre Robin
sequence or syndrome with signs described:
micrognathia, glossoptosis, and obstruction
of the upper airways frequently associated
with a palatal cleft (e.g., Cladis et al., 2014;
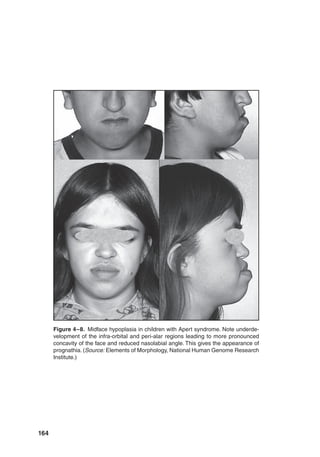
Figure 4–7. A. Frontal view of an infant with Apert syndrome. Note midface hypo-
plasia in the infant and syndactyly of the affected parent holding the child. B. Lateral
view of infant with Apert syndrome. (Source: From Volk, M. S., Arnold, S., Brod-
sky, L. Otolaryngology and audiology. In L. Brodsky, L. Holt, D. H. Ritter-Schmidt
[Eds.], Craniofacial anomalies: An interdisciplinary approach [p. 172]. St. Louis, MO:
Mosby-Year Book. Copyright 1992 by Mosby-Year Book. Reprinted by permission.)
A B](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-180-320.jpg)
![165
Figure 4–9. Lateral neck radiograph of infant in Figure 4–7.
Note maxilla impacted on skull base and the absence of a
nasopharynx.(Source: From Volk, M.S., Arnold, S., Brodsky,
L. Otolaryngology and audiology. In L. Brodsky, L. Holt, D. H.
Ritter-Schmidt [Eds.], Craniofacial anomalies: An interdisciplin-
ary approach [p. 172]. St. Louis, MO: Mosby-Year Book. Copy-
right 1992 by Mosby-Year Book. Reprinted by permission.)
Figure 4–10. Glossoptosis. Note the tongue’s posterior placement
in the oral cavity and the presence of the formula. (Source: https://
elementsofmorphology.nih.gov/index.cgi?tid=ddc1a2c7e23644e8)](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-182-320.jpg)
![166 Pediatric Swallowing and Feeding: Assessment and Management
Giudice et al., 2018). Some children have
airway obstruction at rest that includes stri-
dor, retractions, and cyanosis. In other chil-
dren, obstruction may be subtle in its pre-
sentation and not manifest until feeds are
introduced. Grunting, choking, and cough-
ing with prolonged, difficult feeds may indi-
cate airway compromise. The mechanisms
can vary among patients, but three basic
mechanisms have been described and can
be identified using FFNL. The most com-
mon mechanism for obstruction is glos-
soptosis at the level of the hypopharynx
during inspiration. On occasion, the palatal
shelves of the cleft may be drawn medially
to obstruct the airway. At other times, lat-
eral pharyngeal wall hypotonia may cause
pharyngeal/hypopharyngeal collapse (Giu-
dice et al., 2018; Shprintzen, 1988).
Treatment of the airway obstruction
in nonsyndromic Pierre Robin sequence
depends on the anatomic location of the ob-
struction. Treatment options (Khansa et al.,
2017) include watchful waiting for growth
and development in mildly affected cases,
nasopharyngeal tubes, stenting, prone posi-
tioning (Delorme, Laroque, Caouette-
Laberge, 1989), glossopexy (tongue-lip
adhesion [TLA]) (Argamaso, 1992; Great-
house et al., 2016; Viezel-Mathieu, Safran,
Gilardino, 2016), mandibular distrac-
tion osteogenesis (MDO; Figure 4–11)
(Breik, Umapathysivam, Tivey, Ander-
son, 2016; Jenny, Massenburg, Weissler,
Taub, 2017; Khansa et al., 2017), and tra-
cheostomy. Multiple reports of outcomes
following TLA, MDO, and conservative
management stress that patient selection
to determine surgical need and the most
appropriate surgical procedure is a critical
factor in comparing outcomes. Overall, it
appears that MDO demonstrates superior
outcome measures at 1 month and 1 year
compared to TLA (Flores et al., 2014; Great-
house et al., 2016). Papoff and colleagues
(2013) found that infants with severe air-
way obstruction related to PRS can benefit
safely from either TLA or MDO. MDO sta-
bilizes airway patency more efficiently with
full oral feeding achieved more rapidly than
with TLA. It is important to note that not
all mandibular hypoplasias are manifesta-
tions of the Pierre Robin sequence. Accurate
diagnosis is essential for the development of
long-term treatment plans and for predict-
ing prognosis. A genetics or dysmorphology
Figure 4–11. Pre- and post-mandibular distraction osteogenesis (MDO) for mandibular
hypoplasia manifestations of Pierre Robin sequence.The infant was fed by nasogastric
tube before distraction. (Source: Courtesy of Jordan Steinberg, MD.)
A B](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-183-320.jpg)






![174 Pediatric Swallowing and Feeding: Assessment and Management
including cardiovascular, GI, and urologic
anomalies. In patients with laryngeal clefts,
esophageal atresia and tracheoesophageal
fistula have been reported in 20% to 37% of
patients (Evans, Courteney-Harris, Bailey,
Evans, Parsons, 1995; Mahour, Cohen,
Woolley, 1973). Similarly, in a series of
139 patients with tracheoesophageal fistula/
esophageal atresia, approximately 25% of
patients had a concomitant laryngeal cleft
(Hseu et al., 2015).
Signs and symptoms of laryngeal cleft
pathology vary with approximately 50%
presenting with swallowing deficits, 37%
with respiratory symptoms, and 47% with
laryngeal or pharyngeal symptoms such
as voice disturbance of pharyngeal hyper-
secretion (Adil, Gergin, Kawai, Rahbar,
Watters, 2016; Pezzettigotta, Leboulanger,
Roger, Denoyelle, Garabedian, 2008; Rah-
bar et al., 2006).
Signs and Symptoms of Laryngeal
Clefts. Signs/symptoms related to laryn-
geal clefts reflect the depth of the defect.
n Type 1 laryngeal clefts present with
significant variability, and symptoms
are related to the effects of laryngeal
penetration or aspiration (Figure 4–20).
In general, type 1 laryngeal clefts may be
silent or present with mild to moderate
Figure 4–19. Benjamin and Inglis’ original classification. Type I: supraglottic, interarytenoid
cleft, above the vocal fold level. Type II: cleft extending below the vocal folds into the cricoid
cartilage.Type III: cleft extending through the cricoid cartilage and into the cervical trachea.Type
IV: cleft extending into the thoracic trachea, potentially down to the carina. (Source: Reprinted
with permission from Benjamin, B., Inglis, A. [1989]. Minor congenital laryngeal clefts: Diag-
nosis and classification. Annals of Otology, Rhinology, and Laryngology, 98(6), 417–420.
doi:10.1177/000348948909800603)](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-191-320.jpg)










![4. The Upper Airway and Swallowing 185
congenital anomaly. Ear, Nose and Throat
Journal. 77:1, 51–55.
Breik, O., Umapathysivam, K., Tivey, D.,
Anderson, P. (2016). Feeding and reflux
in children after mandibular distraction
osteogenesis for micrognathia: A systematic
review. International Journal of Pediatric Oto-
rhinolaryngology, 85, 128–135. doi:10.1016/j
.ijporl.2016.03.033
Brody, A., Kuhn, H., Seidel, F. G., Brodsky, L.
(1991). Ultrafast CT evaluation of the airway
in children. Pediatric Radiology, 178, 181–184.
Carr, M. M., Nguyen, A., Poje, C., Pizzuto, M.,
Nagy, M., Brodsky, L. (2000). Correlation of
findingsondirectlaryngoscopyandbronchos-
copy with presence of extraesophageal reflux
disease. Laryngoscope, 110(9), 1560–1562.
doi:10.1097/00005537-200009000-00030
Carter, J. M., Lawlor, C., Guarisco, J. L. (2014).
The efficacy of mitomycin and stenting in
choanal atresia repair: A 20-year experience.
International Journal of Pediatric Otorhino-
laryngology, 78(2), 307–311.
Carter, J., Rahbar, R., Brigger, M., Chan, K.,
Cheng, A., Daniel, S. J., . . . Thompson, D.
(2016). International Pediatric ORL Group
(IPOG) laryngomalacia consensus recom-
mendations. International Journal of Pediat-
ric Otorhinolaryngology, 86, 256–261. doi:10
.1016/j.ijporl.2016.04.007.
Cedin, A. C., Atallah, A. N., Andriolo, R. B.,
Cruz, O. L., Pignatari, S. N. (2012). Surgery
for congenital choanal atresia. Surgery for
congenital choanal atresia. Cochrane Data-
base of Systematic Reviews, (2), CD008993.
doi:10.1002/14651858.CD008993.pub2
Chun, R. H., Wittkopf, M., Sulman, C., Arved-
son, J. (2014). Transient swallowing dysfunc-
tion in typically developing children follow-
ing supraglottoplasty for laryngomalacia.
International Journal of Pediatric Otorhino-
laryngology, 78(11), 1883–1885.
Chun, R. H., Wittkopf, M., Sulman, C., Arved-
son, J. (2015). Corrigendum to “Transient
swallowing dysfunction in typically devel-
oping children following supraglottoplasty
for laryngomalacia” [International Journal
of Pediatric Otorhinolaryngology, 78, 1883–
1885]. International Journal of Pediatric Oto-
rhinolaryngology, 79(12), 2489. doi:10.1016/j
.ijporl.2015.10.004
Cladis, F., Kumar, A., Grunwaldt, L., Otteson, T.,
Ford, M., Losee, J. E. (2014). Pierre Robin
Sequence: A perioperative review. Anesthesia
and Analgesia, 119(2), 400-412. doi:10.1213/
ANE.0000000000000301
Clayburgh, D., Milczuk, H., Gorsek, S., Sinden,
N., Bowman, K., MacArthur, C. (2011).
Efficacy of tonsillectomy for pediatric pa-
tients with dysphagia and tonsillar hyper-
trophy. Archives of Otolaryngology-Head and
Neck Surgery, 137(12), 1197–1202. doi:10
.1001/archoto.2011.196
Cohn, E. C., Robertson, T. S., Scott, S. A., Finley,
A. M., Huang, R., Miles, D. K. (2018). Extu-
bation failure and tracheostomy placement
in children with acute neurocritical illness.
Neurocritical Care, 28(1), 83–92. doi:10.1007/
s12028-017-0429-0
Conley,S.F.,Beecher,R.B.,Delaney,A.L.,Norins,
N. A., Simpson, P. M., Li, S. H. (2009). Out-
comes of tonsillectomy in neurologically
impaired children. Laryngoscope, 119(11),
2231–2241. doi:10.1002/lary.20600
Czechowicz, J. A., Chang, K. W. (2014). Analy-
sis of growth curves in children after adeno-
tonsillectomy. JAMA Otolaryngology-Head
and Neck Surgery, 140(6), 491–496. doi:10
.1001/jamaoto.2014.411
Delorme, R., Laroque, Y., Caouette-Laberge, L.
(1989). Innovative surgical approach for the
Pierre Robin anomalad: Subperiosteal release
of the floor of the mouth musculature. Plastic
and Reconstructive Surgery, 83, 960–964.
DeMauro, S. B., D’Agostino, J. A., Bann, C.,
Bernbaum, J., Gerdes, M., Bell, E. F., . . . Kir-
palani, H. (2014). Developmental outcomes
of very preterm infants with tracheostomies.
Journal of Pediatrics, 164(6), 1303–1310.e2.
doi:10.1016/j.jpeds.2013.12.014
Derkay, C. S., Grundfast, K. (1991). Airway
compromise from nasal obstruction in neo-
nates and infants. International Journal of
Pediatric Otorhinolaryngology, 21, 255–257.
Devambez, M., Delattre, A., Fayoux, P. (2009).
Congenital nasal pyriform aperture stenosis:](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-202-320.jpg)
![186 Pediatric Swallowing and Feeding: Assessment and Management
Diagnosis and management. Cleft Palate Cra-
niofacial Journal, 46(3), 262–267.
Dickson, J. M., Richter, G. T., Meinzen-Derr, J.,
Rutter, M. J., Thompson, D. M. (2009). Sec-
ondary airway lesions in infants with laryn-
gomalacia. Annals of Otology, Rhinology, and
Laryngology, 118(1), 37–43. doi:10.1177/
000
348940911800107
Dobbelsteyn, C., Peacocke, S. D., Blake, K., Crist,
W., Rashid, M. (2008). Feeding difficulties
in children with CHARGE syndrome: Preva-
lence, risk factors, and prognosis. Dysphagia,
23(2), 127–135.
Durvasula, V. S., Lawson, B. R., Bower, C. M.,
Richter, G. T. (2014). Supraglottoplasty
outcomes in neurologically affected and
syndromic children. JAMA Otolaryngology-
Head and Neck Surgery, 140(8), 704–711.
doi:10.1001/jamaoto.2014.983
Eibling, D. E., Gross, R. D. (1996). Subglottic
air pressure: A key component of swallowing
efficiency. Annals of Otorhinology and Laryn-
gology, 105, 253–258.
Eladl, H. M., Khafagy, Y. W. (2016). Endo-
scopic bilateral congenital choanal atre-
sia repair of 112 cases, evolving concept
and technical experience. International Jour-
nal of Pediatric Otorhinolaryngology, 85,
40–45.
Emami, A. J., Brodsky, L., Pizzuto, M. (1996).
Neonatal septoplasty: Case report and review
of the literature. International Journal of Pedi-
atric Otorhinolaryngology, 35, 271–275.
Eustaquio, M., Lee, E. N., Digoy, G. P. (2011).
Feeding outcomes in infants after supra-
glottoplasty. Otolaryngology-Head and Neck
Surgery, 145(5), 818–822. doi:10.1177/
0194
599811414513
Evans, K. L., Courteney-Harris, R., Bailey, C. M.,
Evans, J. N., Parsons, D. S. (1995). Man-
agement of posterior laryngeal and laryngo-
tracheoesophageal clefts. Archives of Otolar-
yngology-Head and Neck Surgery, 121(12),
1380–1385.
Flores, R. L., Tholpady, S. S., Sati, S., Fairbanks,
G., Socas, J., Choi, M., Havlik, R. J. (2014).
The surgical correction of Pierre Robin
sequence: Mandibular distraction osteogen-
esis versus tongue-lip adhesion. Plastic and
Reconstructive Surgery,133(6), 1433–1439.
doi:10.1097/PRS.0000000000000225
Funk, R. T., Jabbour, J., Robey, T. (2015). Fac-
tors associated with tracheotomy and decan-
nulation in pediatric bilateral vocal fold
immobility. International Journal of Pediatric
Otorhinolaryngology, 79(6), 895–899. doi:10
.1016/j.ijporl.2015.03.026
Gaude, G. S. (2009). Pulmonary manifestations
of gastroesophageal reflux disease. Annals of
Thoracic Medicine, 4(3), 115–123. doi:10.41
03/1817-1737.53347
Genther, D. J., Skinner, M. L., Bailey, P. J., Capone,
R. B., Byrne, P. J. (2015). Airway obstruction
after lingual frenulectomy in two infants with
Pierre-Robin sequence. International Journal
of Pediatric Otorhinolaryngology, 79(9), 1592–
1594. doi:10.1016/j.ijporl.2015.06.035
Giudice, A., Barone, S., Belhous, K., Morice, A.,
Soupre, V., Bennardo, F., . . . Picard, A. (2018).
Pierre Robin Sequence: A comprehensive
narrative review of the literature over time.
Journal of Stomatology, Oral and Maxillofa-
cial Surgery, 119, 419–428. doi:10.1016/j.jor
mas.2018.05.002
Goldstein, S. J., Wu, R. H., Thorpy, M. J., Shprint-
zen, R. J., Marion, R. E., Saenger, P. (1987).
Reversibility of deficient sleep entrained
growth hormone secretion in a boy with
achondroplasia and obstructive sleep apnea
[published erratum appears in Acta Endocri-
nol (Copenh), 116, 568]. Acta Endocrinologica
(Copenhagen), 116, 95–101.
Governale, L. S. (2015). Craniosynostosis. Pedi-
atric Neurology, 53(5), 394–401. doi:10.1016/j
.pediatrneurol.2015.07.006
Greathouse, S. T., Costa, M., Ferrera, A., Tahiri,
Y., Tholpady, S. S., Havlik, R. J., Flores, R.
L. (2016). The surgical treatment of Robin
sequence. Annals of Plastic Surgery, 77(4),
413–419.
Gulşen, S., Baysal, E., Celenk, F., Aytaç, I.,
Durucu, C., Kanlikama, M., Mumbuç, S.
(2017). Treatment of congenital choanal atre-
sia via transnasal endoscopic method. Journal
of Craniofacial Surgery, 28(2), 338–342.
Halstead, L. (1999). Role of gastroesophageal
reflux in pediatric upper airway disorders.
Head and Neck Surgery, 120, 208–214.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-203-320.jpg)


![4. The Upper Airway and Swallowing 189
the laryngeal closure reflex. Laryngoscope, 87,
1428–1433.
Schumacher, R. E., Weinfeld, I. J., Bartlett,
R. H. (1989). Neonatal vocal cord paralysis
following extracorporeal membrane oxygen-
ation. Pediatrics, 84(5), 793–796.
Shprintzen, R. (1988). Pierre Robin, microgna-
thia and airway obstruction: The dependency
of treatment on accurate diagnosis. Interna-
tional Anesthesiology Clinics, 26, 64–71.
Stagnaro, N., Rizzo, F., Torre, M., Cittadini, G.,
Magnano, G. (2017). Multimodality imag-
ing of pediatric airways disease: Indication
and technique. Radiology Medicine, 122(6),
419–429.
Strychowsky, J. E., Kawai, K., Moritz, E., Rah-
bar, R., Adil, E.A. (2015). To stent or not to
stent? A meta-analysis of endonasal congeni-
tal bilateral choanal atresia repair. Laryngo-
scope, 126(1), 218–227. doi:10.1007/s11547-
017-0737-7
Sultan, B., Lefton-Greif, M. A., Brown, D. J.,
Ishman, S. L. (2009). Congenital nasal pyri-
form aperture stenosis: Feeding evaluation
and management. International Journal of
Pediatric Otorhinolaryngology, 73(8), 1080–
1084. doi:10.1016/j.ijporl.2009.03.026
Thompson, D. M. (2007). Abnormal senso-
rimotor integrative function of the larynx
in congenital laryngomalacia: A new theory
of etiology. Laryngoscope, 117(6 Pt. 2, Suppl.
114), 1–33.
Thompson, D. M. (2010). Laryngomalacia: Fac-
tors that influence disease severity and out-
comes of management. Current Opinions in
Otolaryngology-Head and Neck Surgery, 18,
564–570.
Thottam, P. J., Georg, M., Chi, D., Mehta, D. K.
(2016). Outcomes and predictors of surgical
management in type 1 laryngeal cleft swal-
lowing dysfunction. Laryngoscope, 126(12),
2838–2842. doi:10.1002/lary.26069
Truong, M. T., Messner, A. H., Kerschner, J. E.,
Scholes, M., Wong-Dominguez, J., Milczuk,
H. A., Yoon, P. J. (2007). Pediatric vocal fold
paralysis after cardiac surgery: Rate of recov-
ery and sequelae. Otolaryngology-Head and
Neck Surgery, 137(5), 780–784. doi:10.1016/j
.otohns.2007.07.028.
Tsai, Y. T., Lee, L. A., Fang, T. J., Li, H. Y. (2013).
Treatment of vallecular cysts in infants with
and without coexisting laryngomalacia using
endoscopic laser marsupialization: Fifteen-
year experience at a single-center. Interna-
tional Journal of Pediatric Otorhinolaryngol-
ogy, 77(3), 424–428.
Viezel-Mathieu, A. Safran, T., Gilardino, M.
S. (2016). A systematic review of the effec-
tiveness of tongue lip adhesion in improving
airway obstruction in children with Pierre
Robin sequence. Journal of Craniofacial Sur-
gery, 27(6), 1453–1456.
Vilaplana, F., Muiños, S. J., Nadal, J., Elizalde, J.,
Mojal, S. (2015). Stickler syndrome. Epi-
demiology of retinal detachment. [Article
in English, Spanish]. Archives de la Sociedad
Espanola Oftalmologia, 90(6), 264–268. doi:
10.1016/j.oftal.2014.11.001
Wentland, C., Hersh, C., Sally, S., Fracchia, M. S.,
Hardy, S., Liu, B., . . . Hartnick, C. J. (2016).
Modified best-practice algorithm to reduce
the number of postoperative videofluoro-
scopic swallow studies in patients with type 1
laryngeal cleft repair. JAMA Otolaryngology-
Head and Neck Surgery, 142(9), 851–856.
doi:10.1001/jamaoto.2016.1252
Yeung, J. C., Balakrishnan, K., Cheng, A. T. L.,
Daniel, S. J., Garabedian, E. N., Hart, C. K.,
. . . Rahbar, R. (2017). International Pediatric
Otolaryngology Group: Consensus guide-
lines on the diagnosis and management of
type I laryngeal clefts. International Journal
of Pediatric Otorhinolaryngology, 101, 51–56.
doi:10.1016/j.ijporl.2017.07.016](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-206-320.jpg)

























































![248 Pediatric Swallowing and Feeding: Assessment and Management
data with population data. Hence, z-scores
are now recommended for the assessment
of nutritional status in children (Mehta
et al., 2013). A z-score represents the num-
ber of standard deviations that a specific
data point is above or below the mean (or
50th percentile). The 50th percentile is
equal to a z-score of 0, and so data points
above the 50th percentile are positive while
data points below the 50th percentile are
negative. The second percentile is roughly
a z-score of −2, while the 98th percentile is
roughly a z-score of +2. The 25th and 75th
percentiles are −0.67 and +0.67, respectively.
Z-scores can be used to describe children
under the first (or over the 99th) percentile
and should be used to describes changes in
anthropometric data over time (e.g., a drop
from the 50th percentile [z-score: 0] to the
25th percentile [z-score: −0.67] is a drop in
0.67 z-scores).
Mid-upper arm circumference (MUAC)
for age z-score has become a recommended
indicator for monitoring nutrition sta-
tus. It is a primary indicator for diagno-
sis and documentation of undernutrition
and should be used in the care of children
(Becker et al., 2015). WHO standards are
recommended for children 6 to 59 months
of age (de Onis, Yip, Mei, 1997). For chil-
dren older than 59 months, standard devia-
tions have recently been reported (Abdel-
Rahman, Bi, Thaete, 2017). MUAC has
been shown to be more sensitive to changes
in fat and muscle mass than BMI in adults
(Powell-Tuck Hennessy, 2003).
In sick premature infants, weight mea-
sures are recommended daily. Length and
head circumference are measured weekly.
Changes in fluid balance occur rapidly in
these premature infants and can greatly
alter body weight, so trends in growth over
time are important. Appropriate growth is
measured by an increase in all body com-
partments. Unfortunately, standards are
not available for triceps skin fold or MUAC
measurements in premature infants or for
infants up to 3 months of age.
Full-term infants should be weighed
to the nearest 0.01 kg with no diaper or a
dry diaper on a table beam or digital infant
scale (Figure 6–5). Older children should be
weighed to the nearest 0.1 kg with little or
no outer clothing and no shoes (Figure 6–6).
Length is measured to the nearest
0.1 cm. Children less than 2 years of age
are measured in supine position. Lengths
should be obtained with the infant in supine
position on a measuring board, with the
Figure 6–4. Physical exam area for identifi-
cation of muscle loss. Patellar region—quad-
ricep muscle.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-265-320.jpg)















![7. Clinical Swallowing and Feeding Assessment 265
for affected children is challenging. Clini-
cians may find it helpful to consider three
interrelated concepts—critical thinking,
clinical reasoning, and clinical judgment
(Victor-Chmil, 2013).
Critical thinking refers to cognitive
processes for the analysis of information
derived from evidence and science rather
than assumptions or conjectures. When
acquiring knowledge, clinicians need to
judge the type and credibility of sources and
recognize the impact of any of their biases
or those related to the source of informa-
tion (Hayes, Chatterjee, Schwartzstein,
2017; Schwartzstein Parker, 2011). Pri-
mary sources of information appear as
original research articles in peer-reviewed
journals. When determining the utility of
these articles, clinicians are urged to con-
sider the study design, population studied,
statistical analysis, appropriateness of the
methodology, and whether the data support
the conclusions. Secondary sources include
textbooks and review articles. These sources
of information were created by authors
who interpret information from a range of
sources (e.g., primary or anecdotal). Cli-
nicians are encouraged to determine the
appropriateness of citations and presence
of potential of intentional or unintentional
author biases (Schwartzstein Parker,
2011). Consensus statements, white papers,
and credible websites (e.g., PubMed.gov
[https://www.ncbi.nlm.nih.gov/pubmed]
or Online Mendelian Inheritance in Man
[OMIM, https://www.omim.org/]) pro-
vide information from a panel of experts to
inform readers about complex information
and to guide problem-solving and decision-
making. Nonetheless, clinicians need to
determine whether the reported informa-
tion is relevant to their patient population
and to be aware of the biases and scope of
evidence reviewed by the group issuing the
report. Finally, social media and professional
and support groups have become a means
of obtaining information. Again, clinicians
are advised to consider the source of the
information reported (e.g., primary or anec-
dotal), biases, and the transparency of finan-
cial disclosures. Critical thinking is used to:
n define a patient’s problem,
n gather and analyze patient information,
n examine the evidence-based practice in
caring for the patient,
n evaluate the relevance of the informa-
tion, and
n decide on possible “discipline-specific”
actions to improve the patient’s
physiologic and psychosocial outcomes
(Connors Siner, 2015; Foundation for
Critical Thinking, n.d.; Tanner, 2006;
Victor-Chmil, 2013).
The term clinical reasoning refers to the
application of the information (derived dur-
ing the critical thinking process) to the clin-
ical situation for an individual patient. Clin-
ical reasoning requires the integration of the
“best data” for the identification of the most
appropriate interventions that will improve
the specific patient’s condition. It requires
the ability to sort through a cluster of fea-
tures presented by a patient and accurately
assign a diagnostic label, with the develop-
ment of an appropriate treatment as an end
goal (Connors Siner, 2015; Foundation
for Critical Thinking, n.d.; Tanner, 2006).
The key elements of clinical reasoning are
knowledge, skill or experience, and context
(e.g., professional or institutional wisdom
and culture) (Bowen, 2006).
Clinical judgment refers to decisions
based on “knowing the patient.” Clinical
judgments may include interpretation or
conclusion about a patient’s needs, con-
cerns, or health problems, and decision to
take (or not) actions, use or modify stan-
dard approaches, or improvise new ones
as deemed appropriate by the patient’s
responses (Tanner, 2006).](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-282-320.jpg)



![7. Clinical Swallowing and Feeding Assessment 269
research continues to identify sensitivity
and specificity of relevant items.
Vetted Questionnaires
Vetted questionnaires appear to fall into two
primary categories. First, questionnaires are
directed for families to use to detect pos-
sible problems in their children (e.g., Infant
and Child Feeding Questionnaire (ICFQ)
(Barkmeier-Kramer et al., 2017). Second,
questionnaires are used by medical and
health care professionals (e.g., Dysphagia
Disorder Survey [DDS]) (Sheppard, Hoch-
man, Baer, 2014).
Pediatric Clinic/Bedside
Swallowing and Feeding
Evaluation/Assessment Tools
Little is known about clinical properties
and psychometric soundness of clinical
pediatric oral sensorimotor swallowing and
feeding assessments. Systematic reviews of
assessment tools concluded that overall,
Table 7–3. Red Flags/Key Questions to Aid in Decisions for Referral to Clinical Swallowing
and Feeding Assessment
Questions or
Concerns
Examples of Presentations With Rationale and
Literature Support
Airway/respiratory • Gurgly voice, coughing, and multiple swallows best predictors of
dysphagia (Benfer et al., 2015)
• Repeated chest infections and hospitalizations common signs
of unsafe swallowing (Peterson et al., 2006)
Feeding duration • Longer than 30 minutes frequently or 2.5 hours per day
(Sullivan et al., 2004)
• Greater than 45–60 minutes can lead to malnutrition (Hals, Ek,
Svalastog, Nilsen, 1996; Ramage, Simpson, Thomson,
Patersen, 1997)
Weight gain or lack
of weight gain
• Lack of weight gain over just 2–3 months in children less than
2 years of age like weight loss in older children and adults
• Oral sensorimotor impairment may affect functional capacity of
children and health quality of life (Liu Saltzman, 2009)
GI Retching/vomiting • Up to 77% of children undergoing PEG placement have
histories of vomiting or retching, indicative of GER (Avitsland
et al., 2006)
• PEG insertion does not lead to increased reflux in children with
CP (Kakade, Coyle, McDowell, Gillick, 2015)
Stress at mealtimes • Battles not likely to get child to eat more
• Poor feeding ability is major stress for parents (Sullivan, 2004)
• Stress may be more prominent in parents, the child, or both
Note. CP = cerebral palsy; GER = gastroesophageal reflux; PEG = percutaneous endoscopic gastrostomy.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-286-320.jpg)






![276 Pediatric Swallowing and Feeding: Assessment and Management
children with multiple disabilities (Gisel
Patrick, 1998). Mealtimes should take
approximately 30 min in most cultures. If
on a routine basis 45 to 50 min or more are
required to complete a meal, changes need
to be made to improve the efficiency. The
risk for aspiration increases with the dura-
tion of mealtimes (Arvedson et al., 1994).
Duration of mealtimes also must be consid-
ered in relationship to other activities that
are important in each day. The child should
not expend more energy eating than what
is consumed. Some mothers have reported
spending up to 7 hours a day feeding a
child (Johnson Deitz, 1985). Types of
food refusals are noted (e.g., turning head,
throwing food, expelling/spitting food out
of the mouth, leaving the table). Clinicians
should inquire about more examples or
descriptions of stress involved in mealtimes.
Other considerations include, but are not
limited to, religious and/or cultural factors
that affect family food choices as well as
mealtime habits.
The nutrition status (Chapter 6) and the
interactive behaviors of the caregiver and
childarealsoimportantfactors(Chapter13).
The long-term prognosis for development
of functional oral sensorimotor skills and
safe oral feeding relates directly to the under-
lying health and neurologic status. The infor-
mation gained through thorough history
Table 7–6. Factors Included in a Feeding History for Oral and Nonoral Feeders
Position(s) for feeding and seating arrangements
Duration of feeding times (average and range)
Intervals between feedings or meal times (from start of one feeding to start of next)
Tube feeding (type, partial or total nutrition, nighttime rate if overnight feeds)
Infants: Breast- or bottle-feeding (types of nipples, formula)
Infants burping: Spontaneous? Feeder interrupt to burp?
Children who get food as well as liquid: Types of textures, use of utensils
Child’s participation in self-feeding process (total or assisted)
Diet: At least a 3-day diet history is helpful including all food and liquid with
amounts; permits dietitian to calculate nutritional value and calories
Respiratory status: Aspiration pneumonia, bronchitis, asthma, etc. Noisy
breathing, gurgly voice quality with feeding, coughing, choking
Other signs of distress: Fussy during feeding, food refusal, falling asleep,
arching, neck hyperextension
Other factors: Tests (e.g., upper gastrointestinal study [UGI], esophageal
manometry, endoscopy, scintiscan, pH study, videofluoroscopic swallow
study [VFSS]; flexible endoscopic examination of swallowing (FEES), surgical
procedures, medical treatments, medications)
Sleep patterns: Restless, waking during the night, snoring, mouth breathing
Cognitive and communication status: Verbal and nonverbal skill levels
Behavior during meals: Stress at mealtimes, refusals, participation with family
History of therapeutic intervention for developmental or feeding problems](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-293-320.jpg)
![7. Clinical Swallowing and Feeding Assessment 277
taking is invaluable in planning the rest of
the evaluation. There is no single pediatric
assessmentscalethatcanberecommendedto
encompass all aspects of a clinic swallowing
and feeding evaluation. In some instances,
clinicians may take portions of commercially
available scales and modify them to meet
the needs of their populations, institutions,
or practice patterns. Standardized processes
with reliability and validity are urged as aids
in data collection for research and clinic pur-
poses to provide practice guidelines across
institutions and populations.
Physical Examination
(Prefeeding Assessment)
The clinical examination of swallowing
and feeding for all infants and children
begins with overall observation of the “at
rest” posture and position. The observer
realizes that underlying tone and strength
are particularly important as a basis for
decision-making regarding oral feeding
safety. It is important for all professionals
to do a lot of looking and listening before
focusing on the mouth and feeding. The
initial signs and symptoms of feeding dif-
ficulties may be markers for broader cen-
tral or peripheral nervous system deficits
and closely related to airway and GI tract
function. During prefeeding observations,
clinicians note deviations from “normal”
expectations, even though normative data
are lacking in many aspects of feeding (e.g.,
Arvedson, 2008; Arvedson Rogers, 1993;
Korth Rendell, 2015; Marcus Breton,
2013). Observations should focus on:
n interactions between parents/caregivers
and child;
n posture, position, tone, and movement
patterns, particularly head, neck, and
trunk;
n respiratory patterns (e.g., mouth
breathing to compensate for problem
with nasal breathing, effort [retractions
suprasternal and/or substernal, inspira-
tory stridor as sign of upper airway
obstruction], alterations in rate that
may interfere with feeding or represent
instability);
n overall responsiveness, temperament,
affect;
n alertness, ability to sustain attention to
task;
n response to sensory input (e.g., vestib-
ular, proprioceptive, visual, olfactory,
tactile, auditory); and
n signs of self-regulation, self-calming.
Clinicians must be able to interpret cues
from the child indicating readiness to feed
or not to feed as the case may be.
The overall goals of this assessment are
to determine the nature of the problem
and best possible options for management.
Assessment is not a one-time event but an
ongoing process with caregivers always inte-
gral to both assessment and treatment.
Readiness for Feeding:
Sensorimotor and
Posture Factors
Oral Sensorimotor Assessment
Sensory and motor functions are inter-
twined and must be considered in light of
cranial nerve innervation to the muscles
involved in oral and pharyngeal phases of
swallowing. The cranial nerves that inner-
vate muscles for swallowing all provide
sensory and motor input, except CN XII,
which provides motor control to the intrin-
sic muscles of the tongue (see Chapter 2). As
a result of developmental processes, older
infants and children acquire competence in
discernment of the physical characteristics](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-294-320.jpg)
































![310 Pediatric Swallowing and Feeding: Assessment and Management
neurodevelopmental outcome of an infant
born at 21 weeks’ 4 days’ gestation. Pediatrics,
140(6). doi:10.1542/peds.2017-0103
Alexander, R. (1987). Oral-motor treatment
for infants and young children with cerebral
palsy. Seminars in Speech and Language, 8,
87–100.
Altimier, L., Phillips, R. M. (2013). The Neo-
natal Integrative Developmental Care Model:
Seven neuroprotective core measures for
family-centered developmental care. New-
born and Infant Nursing Reviews, 13(1), 9–22.
American Academy of Pediatrics, American
College of Obstetricians and Gynecologists;
Committee on Fetus and Newborn and
ACOG Committee on Obstetric Practice.
(2017). Guidelines for perinatal care. In S. J.
Kilpatrick, L-A. Papile, G. A. Macones, K.
L. Watterberg (Eds.), Guidelines for perinatal
care (8th ed., p. 221). Elk Grove Village, IL;
Washington, DC: Authors.
American Academy of Pediatrics, A Minute for
Kids, [radio series] WBBM-AM. Chicago, IL.
Retrieved from https://www.aap.org/en-us/
about-the-aap/aap-press-room/aap-press-
room-media-center/Pages/Weaning-from-
the-Bottle.aspx
American Academy of Pediatrics, Task Force on
Infant Positioning and SIDS. (2016, Novem-
ber 9). The new AAP guidelines on SIDS and
safe sleep recommendations. Retrieved from
http://birthperspectives.com/2016/11/09/
the-new-aap-guidelines-on sids-and-safe-
sleep-recommendations/
American Psychiatric Association. (2013). Diag-
nostic and statistical manual of mental disor-
ders (5th ed.). Washington, DC: Author.
Apgar, V. (1966). The newborn (APGAR) scor-
ing system: Reflections and advice. Pediatric
Clinics of North America, 13, 645.
Arens, R., Reichman, B. (1992). Grooved pal-
ate associated with prolonged use of orogastric
feeding tubes in premature infants. Journal of
Oral Maxillofacial Surgery, 50, 64–65.
Arvedson, J. C. (2008). Assessment of pediatric
dysphagia and feeding disorders: Clinical and
instrumental approaches. Developmental Dis-
abilities Research Reviews, 14(2), 118–127.
Arvedson, J. C. (2013). Feeding children with
cerebral palsy and swallowing difficulties.
European Journal of Clinical Nutrition, 67,
S9–S12.
Arvedson, J., Brodsky, L. (2002). Management
of feeding and swallowing problems. In Pedi-
atric swallowing and feeding: Assessment and
management (2nd ed., Rev ed., pp. 389–468).
San Diego, CA: Singular.
Arvedson, J., Clark, H., Lazarus, C., Schooling,
T., Frymark, T. (2010). Evidence-based
systematic review: Effects of oral motor
interventions on feeding and swallowing in
preterm infants. American Journal of Speech
Language Pathology, 19(4), 321–340.
Arvedson, J., Rogers, B. (1993). Pediatric
swallowing and feeding disorders. Journal
of Medical Speech-Language Pathology, 1(4),
203–221.
Arvedson, J., Rogers, B., Buck, G., Smart, P.,
Msall, M. (1994). Silent aspiration prominent
in children with dysphagia. International
Journal of Pediatric Otorhinolaryngology, 28,
173–181.
Avitsland, T. L., Kristensen, C., Emblem, R., Veen-
stra, M., Mala, T., Bjornland, K. (2006).
Percutaneous endoscopic gastrostomy in chil-
dren: A safe technique with major symptom
relief and high parental satisfaction. Journal
of Pediatric Gastroenterology and Nutrition,
43(5), 624–628.
Barkmeier-Kraemer, J. M., Linn, C., Thompson,
H. L., Byrd, R. S., Steinfeld, M. B., Hoffmann,
R. G., Silverman, A. H. (2017). Preliminary
study of a caregiver-based infant and child
feeding and swallowing screening tool. Jour-
nal of Pediatric Gastroenterology and Nutri-
tion, 64, 979–983.
Barton, C., Bickell, M., Fucile, S. (2017). Pedi-
atric oral motor feeding assessments: A sys-
tematic review. Physical and Occupational
Therapy in Pediatrics, 21, 1–20.
Benfer, K., Weir, K., Bell, K., Ware, R., Davies, P.,
Boyd, R. (2013). Oropharyngeal dysphagia
and gross motor skills in children with cere-
bral palsy. Pediatrics, 131, E1553–E1562.
Benfer, K. A., Weir, K. A., Bell, K. L., Ware, R.
S., Davies, P. S., Boyd, R. N. (2015). Clini-](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-327-320.jpg)














![7. Clinical Swallowing and Feeding Assessment 329
Time to finish feeding: 30 minutes 30 minutes Feeding not finished
Amount of intake
Modifications during assessment:
Type
Response
CLINIC ASSESSMENT
Feeding/swallowing disorder may include, be related to, or contribute to problems
with: (Check [3] all that apply)
Airway protection
Nutrition or growth compromise, or gastrointestinal tract
Oral sensorimotor skills
Behavioral responses to mealtimes
Environmental factors (e.g., stress or inconsistent expectations)
Strengths:
Challenges:
PLANS/RECOMMENDATIONS
Oral feeding, tastes, sensorimotor
Oral feeding without modifications or restrictions
Oral feeding with modifications
Oral tastes for pleasure: ______________________
Nonoral feeding with nonnutritive oral stimulation
Other evaluations
Pediatric specialty services: Type:
Instrumental swallowing evaluation: Type:
Other:
Follow-up and interventions (see Chapter 9)](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-346-320.jpg)


![8. Instrumental Evaluation of Swallowing 333
hypopharynx and larynx is critical for
accurate diagnosis in many presentations
of pediatric dysphagia. Use of FEES was
first described by Langmore and colleagues
almost three decades ago (Langmore,
Schatz, Olsen, 1988, 1991).
The endoscopic method for evaluation
of swallowing provides information about
the events occurring immediately before
and immediately after the pharyngeal swal-
low. Hence, compared to videofluoroscopy
(discussed later), the FEES provides infor-
mation that is limited by a period of “white-
out” during the pharyngeal swallow.
Advances in digital video systems and
digital distal chip technology have revolu-
tionized the use of this tool as safe and highly
informative in both the diagnosis and treat-
ment of swallowing dysfunction in patients
of all ages, beginning with preterm infants
(e.g., Plaat, van der Laan, Wedman, Halmos,
Dikkers, 2014). In some instances, FEES
may be an adjunct to VFSS (Bastian, 1991).
Real-time simultaneous integration of FEES
with a VFSS from the same patient has been
facilitated by technology advances.
FEES Procedure
Optimally, FEES is best performed by a
team consisting of a pediatric otolaryn-
gologist and a speech-language pathologist
(SLP). The physician is skilled at passing
the flexible scope and has the comprehen-
sive knowledge base to assess the anatomic,
physiologic, and functional abnormali-
ties found in the nasal, pharyngeal, and
laryngeal regions. The SLP has specialized
knowledge and experience in swallowing
and communication and is able to focus
on the oral sensorimotor status of the child
and functional aspects of swallowing. This
interdisciplinary team approach capitalizes
on the expertise of professionals in these
two allied fields, thereby providing a more
Figure 8–1. Common factors that determine/modify the impact and management
of the feeding/swallowing dysfunction. (Source: Adapted from Lefton-Greif, M. A.,
McGrath-Morrow, S. A. [2007]. Deglutition and respiration: Development, coor-
dination, and practical implications. Seminars in Speech and Language, 28[3],
166–179.)](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-350-320.jpg)



![8. Instrumental Evaluation of Swallowing 337
as VFSS and all medical procedures, find-
ings when patients are stressed and unco-
operative must be interpreted with caution.
The most informative evaluations mimic
the usual swallowing pattern for the patient.
Nonetheless, noncooperative children and
of course infants can be studied with a mod-
icum of information to be gained.
FEES is performed at bedside, includ-
ing in the NICU or in a clinic, and does not
require that children be taken to a radiology
suite. In the NICU, FEES can be performed
with infants who are breastfeeding (Wil-
lette, Molinaro, Thompson, Schroeder,
2016) and as a team assessment (Reynolds,
Carroll, Sturdivant, 2016). FEES is par-
ticularly helpful for children who have diffi-
culties transferring to alternate seating sys-
tems, such as those with severe scoliosis or
kyphosis. These children cannot be exam-
ined easily in the radiology suite either.
Children with muscular dystrophy or other
neuromuscular conditions can be examined
in their typical feeding postures in whatever
seating systems are used at home and school
environments.
Videofluoroscopic
Swallow Study
Videofluoroscopy is the primary imaging
technique for detailed dynamic assessment
of oral, oropharyngeal, pharyngeal, and
upper esophageal phases of a swallow. VFSS
or modified barium swallow (MBS) study
are the two most common terms for swal-
lowing studies that use videofluoroscopic
imaging procedures. A comprehensive eval-
uation of esophageal and lower GI function
(i.e., an esophagram and upper gastrointes-
tinal [UGI] study) requires additional pro-
cedures by a radiologist. The esophagus is
only screened during the VFSS procedure.
VFSS is useful for diagnostic purposes and
to assist in management decisions. Dif-
ferences in handling a variety of textures,
assessment of facilitative and/or compen-
satory techniques, and reeducation proce-
dures are well known (Logemann, 1993;
Martin-Harris, Logemann, McMahon,
Schleicher, Sandidge, 2000).
VFSS is used as part of a comprehen-
sive diagnostic evaluation of infants, includ-
ing premature infants, and children with
suspected swallowing deficits. Although
somewhat of a misnomer, the VFSS is often
referred to as the “gold standard.” This is an
exaggeration because the findings reflect
only a brief window in time in a somewhat
artificial setting. Nonetheless, the informa-
tion obtained when the study is carried out
effectively with a cooperative patient is valu-
able as an important “piece of the puzzle.”
VFSS has been used widely since the
early 1980s (Logemann, 1983), and its use
has been increasing because of the increas-
ing number of children with swallowing
dysfunction (Arvedson, 2008; Lefton-Greif,
2008). The VFSS remains the most compre-
hensive examination for evaluation of pha-
ryngeal function in the swallowing process
and its interface with oral/oropharyngeal
transit and cervical esophageal function.
Cricopharyngeal opening, esophageal
motility, and transit time are screened
when a bolus is followed through the upper
esophageal sphincter (UES) and esophagus.
Radiologic information gained is listed in
Table 8–2 (Arvedson et al., 1994; Arvedson
Lefton-Greif, 1998; Lefton-Greif et al.,
2018; Nordin, Miles, Allen, 2017).
DespitetheincreasinguseofVFSS,ques-
tionshavebeenraisedaboutitsutilityrelative
to justification for the associated exposure to
ionizing radiation. Clinical utility has been
criticized because of the paucity of infor-
mation on standardization of procedures
(e.g., amount and order of presentations](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-354-320.jpg)





![8. Instrumental Evaluation of Swallowing 343
copy equipment, and the complexity of the
information needed from the examination
(Arvedson Lefton-Greif, 2017; Weir et al.,
2007). Patient cooperation and caregiver
involvement can reduce the exposure time.
Even with the most difficult older patient,
clinicians are urged to keep total fluoros-
copy time to no more than 2 or 3 min with
rare exceptions. Therapeutic maneuvers
that include changes in head position or
evaluation of different bolus consistencies
and volumes take longer. Thus, therapeu-
tic maneuvers should be used sparingly
when needed for determination of utility
in making optimal recommendations for
management.
Adjustments in frame rate are used to
minimizeradiationexposure.Currently,con-
tinuous fluoroscopy, a fluoroscopic pulse rate
of 30 frames per second (fps) is considered
necessary/optimal for capturing swallow-
ing impairments (Arvedson Lefton-Greif,
1998; Cohen, 2009). Although lower frame
rates (12.5–25 fps) have been reported, data
suggest that these lower rates are inadequate
for detection of penetration and aspiration
events, which would likely be missed at less
than 30 fps (Cohen, 2008, 2009; Hender-
son, Miles, Holgate, Perryman, Allen,
2016; Weir et al., 2007). Research is needed
to determine the lowest frame rate needed
for obtaining reliable and valid findings,
which yield optimal clinical utility and the
best patient outcomes (Bonilha et al., 2013;
Nordin et al., 2017).
Seating and Positioning
Caregivers and clinicians work together to
achieve a typical feeding position for each
child. If the typical position is different
from an optimal position, the child should
be observed in both positions. In general,
the child’s posture should be one that attains
central alignment. No single definition of
optimal position can be stated because indi-
vidual exceptions may be needed. See Chap-
ters 7 and 9 for seating considerations. Com-
mercial seating and positioning options are
available for infants and children. Seating
possibilities for infants and children neces-
sarily are varied to meet the specific needs of
that child within limitations of the fluoros-
copy equipment that allow for transmission
of images to encompass oral, pharyngeal,
and upper esophageal phases of swallow-
ing (Figure 8–3). Radiopaque objects (e.g.,
metallic head supports, snaps, and zippers),
which are visible in the imaging field, must
be removed because they can obstruct views
of the structures of interest.
Given the space limitations between
the upright table and the fluoroscopy unit
in most pediatric radiology suites (typi-
cally 15–18 inches [38–46 cm]), children
are transferred into special seating arrange-
ments. Seating systems need to be posi-
tioned as close as possible to the imaging
equipment to maximize the quality of the
image and reduce the amount of image
magnification. Wheelchairs, even those for
small children, are usually too wide to fit
between the table and the fluoroscopic tube,
and they are too low to allow for viewing the
oral cavity and pharynx, and especially for
screening the esophagus. Portable fluoros-
copy units are used in some adult facilities
(e.g., long-term care facilities), but they may
or may not be appropriate for infants and
young children. C-arm units may be adapt-
able for older children who need to remain
in their own wheelchairs. Other adaptations
may be possible, depending on specification
of equipment in the radiology suite
Seating systems can be adapted in a vari-
ety of ways to meet the needs of most chil-
dren. Basic stability and central alignment
of the infant or child must be maintained
with whatever modifications are made.
A child with poor head and/or trunk control](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-360-320.jpg)







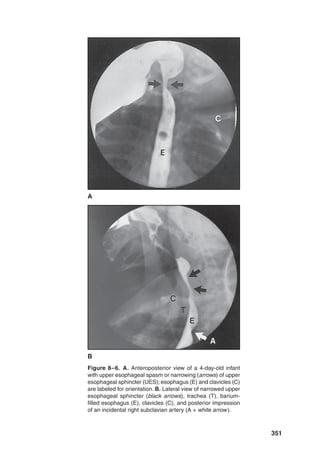






![358 Pediatric Swallowing and Feeding: Assessment and Management
Ultrasound Imaging
of Swallowing
Ultrasound Definitions
and Procedures
US is defined as sound propagated at fre-
quencies above those audible to the human
ear, that is, over 20 kHz. The frequencies
used for diagnostic imaging range between
2 and 10 MHz, a 1,000-fold increase above
the audible range (Sonies, 1991). During US
imaging, a transducer is used both to gener-
ate sound waves and to receive ultrasound
echoes. These echoes are then electronically
converted into computer-generated images.
An ultrasound beam, directed into a soft tis-
sue medium, vibrates tissue particles in that
medium. Body tissues (such as fat, muscle,
and fascia) and fluids (blood, cerebral spinal
fluid, and water) have different densities and
reflect echoes back to the transducer at dif-
ferent intensities, making different tissues
or other substances distinguishable from
each other at their interface. In real time,
US imaging displays movement of anatomic
structures. Doppler is a type of ultrasound
that can detect and measure fluid flow and
has been used to diagnose many medical
conditions (e.g., blood clots, heart valve
defects and congenital heart disease, and
oligohydramnios [insufficient volume of
amniotic fluid during pregnancy]).
Ultrasound with Infant
Breast- and Bottle-Feeding
US has been used to define prenatal predic-
tors of postnatal feeding skills and oral skill
maturation (Miller, Macedonia, Sonies,
2006; Miller, Sonies, Macedonia, 2003).
Doppler images can augment the typical
US images in the fetus by detecting amni-
otic fluid flow and respiratory function
(Macedonia, Miller, Sonies, 2002; Miller
et al., 2006; Miller et al., 2003). US technol-
ogy has been applied to visualize temporal
relationships between movement patterns
of oral and pharyngeal structures in infants
(Bosma, Hepburn, Josell, Baker, 1990;
Smith, Erenberg, Nowak Franken, 1985;
Weber, Woolridge, Baum, 1986) as well
as in older children and adults (Fanucci,
Cerro, Ietto, Brancaleone, Berardi, 1994;
Shawker, Sonies, Hall, Baum, 1983, 1984;
Sonies, 1990; Stone Shawker, 1986; Yang,
Loveday, Metreweli, Sullivan, 1997).
During the postnatal periods, US is
most helpful in describing bolus formation
and oral transit, particularly in bottle- or
breastfed infants (Bosma et al., 1990; Ged-
des Sakalidis, 2016; McClellan, Sakalidis,
Hepworth, Hartmann, Geddes, 2010). In
addition, US imaging has the potential to
track the maturation of sucking patterns in
the early postpartum period and distinguish
between tongue actions associated with
nutritive and nonnutritive sucking (Sakali-
dis et al., 2013).
US imaging is particularly useful when
there is concern for an oral problem during
breastfeeding. Both mother and infant can
be observed for extended time periods to
define the oral function without concern for
radiation exposure in contrast to VFSS (as
previously discussed). For example, when a
breastfeeding infant fails to initiate sucking
readily or shows incoordinated sucking, it
is possible to observe whether the difficulty
is with the infant’s suck–swallow patterns or
the maternal milk supply (McClellan et al.,
2010; Smith et al., 1985). Muscle interac-
tions and nipple deformation must be
functional for successful oral feeding; these
are both clearly seen with US (Sakalidis
et al., 2013).](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-375-320.jpg)



![362 Pediatric Swallowing and Feeding: Assessment and Management
that may interfere with safe oral feeding. She
also demonstrates the importance of under-
standing the impact of “normal” findings
(e.g., nasopharyngeal reflux) on feeding.
Nurses implemented guidelines for maxi-
mizing efficiency of nipple-feeding with
greater confidence once they had the VFSS
findings. The foster parents were trained
to carry out feedings with the best tech-
niques for posture, position, monitoring of
flow rate, and pacing as needed. This infant
grew well over the next several months of
life and made good developmental progress
as anticipated for infants with Grade II IVH.
References
Allen, J. E., White, C. J., Leonard, R. J., Belaf-
sky, P. C. (2010). Prevalence of penetration
and aspiration on videofluoroscopy in nor-
mal individuals without dysphagia. Otolaryn
gology-Head and Neck Surgery, 142(2), 208–
213. doi:10.1016/j.otohns.2009.11.008
Alzen, G., Benz-Bohm, G. (2011). Radiation
protection in pediatric radiology. Deutsches
Arzteblatt International, 108(24), 407–414.
doi:10.3238/arztebl.2011.0407
American College of Radiology. ACR-SPR Prac-
tice Parameter for the Performance of the
Modified Barium Swallow (Revised 2017).
Retrieved from https://www.acr.org/-/media/
ACR/Files/Practice-Parameters/modified-
ba-swallow.pdf
American Speech–Language–Hearing Associa-
tion. (2000). Clinical indicators for instru-
mental assessment of dysphagia (guidelines).
ASHA, (Suppl. 20), 18–19.
American Speech-Language-Hearing Asso-
ciation. (2016). Scope of practice in speech-
language pathology [Scope of practice]. Re-
treived from https://www.asha.org/policy/
Arvedson, J. C. (2008). Assessment of pediatric
dysphagia and feeding disorders: Clinical and
instrumental approaches. Developmental Dis-
abilities Research Reviews, 14(2), 118–127.
Arvedson, J. C., Lefton-Greif, M. A. (1998).
Pediatric videofluoroscopic swallow studies:
A professional manual with caregiver guide-
lines. San Antonio, TX: Communication Skill
Builders/Psychological Corporation.
Arvedson, J. C., Lefton-Greif, M. A. (2017).
Instrumental assessment of pediatric dyspha-
gia. Seminars in Speech and Language, 38(2),
135–146. doi:10.1055/s-0037-1599111
Arvedson, J., Rogers, B., Buck, G., Smart, P.,
Msall, M. (1994). Silent aspiration prominent
in children with dysphagia. International
Journal of Pediatric Otorhinolaryngology, 28,
173–181.
Aviv, J. E., Murry, T., Zschommler, A., Cohen,
M., Gartner, C. (2005). Flexible endoscopic
evaluation of swallowing with sensory test-
ing: Patient characteristics and analysis of
safety in 1,340 consecutive examinations.
Annals of Otology, Rhinology, and Laryngol-
ogy, 114, 173–176
Banno, H., Katsuno, M., Suzuki, K., Tanaka,
S., Suga, N., Hashizume, A., . . . Sobue, G.
(2017). Swallowing markers in spinal and
bulbar muscular atrophy. Annals of Clinical
and Translational Neurology, 4(8), 534–543.
doi:10.1002/acn3.425
Bastian, R. W. (1991). Videoendoscopic evalua-
tion of patients with dysphagia: An adjunct
to the modified barium swallow. Otolaryngol-
ogy-Head and Neck Surgery, 104(3), 339–350.
Beck, T. J., Gayler, B. W. (1990). Image quality
and radiation levels in videofluoroscopy for
swallowing studies: A review. Dysphagia, 5,
119–128.
Bonilha, H. S., Humphries, K., Blair, J., Hill, E.
G., McGrattan, K., Carnes, B., . . . Martin-
Harris, B. (2013). Radiation exposure time
during MBSS: Influence of swallowing im-
pairment severity, medical diagnosis, clini-
cian experience, and standardized protocol
use. Dysphagia, 28(1), 77–85. doi:10.1007/
s00455-012-9415-z
Bosma, J. F., Hepburn, L. G., Josell, S. D.,
Baker, K. (1990). Ultrasound demonstration
of tongue motions during suckle feeding.
Developmental Medicine and Child Neurol-
ogy, 32, 223–229.](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-379-320.jpg)








![372 Pediatric Swallowing and Feeding: Assessment and Management
fundamental to EBM to achieve improve-
ments in patient care and outcomes (Weiner
Sauter, 2003). In 1996, Sackett and col-
leagues defined EBM as the “conscientious,
explicit, and judicious use of the current
best evidence in making decisions about the
care of individual patients” (Sackett, Rosen-
berg, Gray, Haynes, Richardson, 1996).
Over time, the tenets of EBM have been
adopted by many professionals, who refer
to it as evidence-based practice (EBP). A
primary principle of EBP is to offer patients
treatments that do more good than harm
and that are worth the efforts and cost of
using them. The American Speech-Lan-
guage-Hearing Association (ASHA) web-
site operationalized the definition of EBP
as “the integration of: (a) clinical expertise/
expert opinion, (b) external scientific evi-
dence, and (c) client/patient/caregiver per-
spectives to provide high-quality services
reflecting the interests, values, needs, and
choices of the individuals we serve” (https://
www.asha.org/Research/EBP/Introduc-
tion-to-Evidence-Based-Practice/; also
see: https://www.asha.org/Research/EBP/
Framing-the-Clinical-Question/).
Clinically, EBP is an indispensable safe-
guard against pseudoscience and poten-
tially the use of harmful assessment and
treatment methods (Lee Hunsley, 2015).
Importantly, even interventions that appear
to be plausible can be ineffective or exert
iatrogenic consequences (Lee Hunsley,
2015), and all interventions are associ-
ated with costs (e.g., time, money, and/or
energy). Unfortunately, objective data sup-
porting management in pediatric swallow-
ing and feeding disorders are limited and
often devoid of information that identifies
efficacious treatments. Nonetheless, clini-
cians are encouraged to review information
pertinent to their patients from credible
sources including but not limited to consen-
sus statements, white papers, and trustwor-
thy websites (e.g., PubMed [https://www
.ncbi.nlm.nih.gov/pubmed/] and OMIM
[https://www.ncbi.nlm.nih.gov/omim/]).
Frameworks for Management
Decision-Making
World Health Organization’s
International Classification
of Functioning,
Disability, and Health
The International Classification of Func-
tioning, Disability, and Health (ICF) model
is the World Health Organization’s (WHO)
approved classification of health and health-
related domains, which has shifted assess-
ment and treatment paradigms from focus-
ing on impairments to focusing on function
in the broad sense of participation (see
Chapters 1 and 7). As a bio-psychosocial
model, the ICF includes body functions/
structures, activities, participation, and
environmental and personal (social) factors.
Although all children with swallowing and
feeding disorders may exhibit a common
core set of factors, individual profiles (e.g.,
the ability to participate in meals at home,
in school, or in a restaurant) are likely to
be dependent on features unique to the
affected person (e.g., underlying diagnostic
condition, age/developmental status, and
severity of the dysphagia) (Schiariti, Mahdi,
Bolte, 2018). At this time, ICF-based tools
that provide](https://image.slidesharecdn.com/pediatricswallowingandfeedingassessmentandmanagementthird-230503045947-17ccc26b/85/Pediatric_Swallowing_and_Feeding_Assessment_and_Management-_Third-pdf-389-320.jpg)

























































































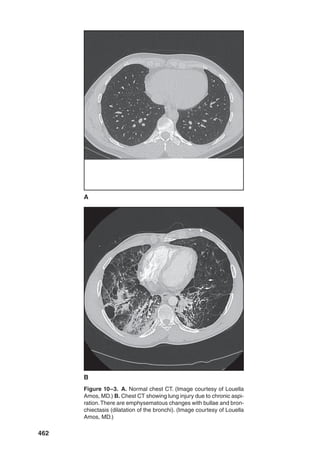






















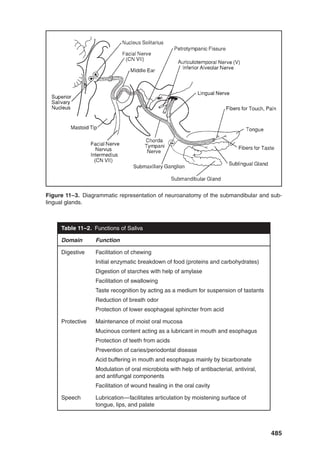



























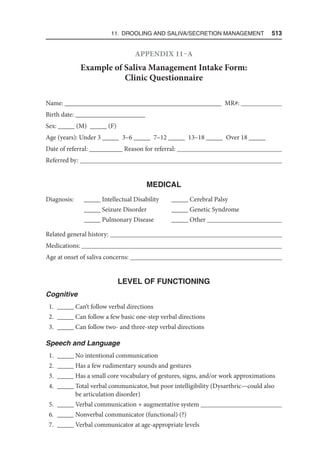





















































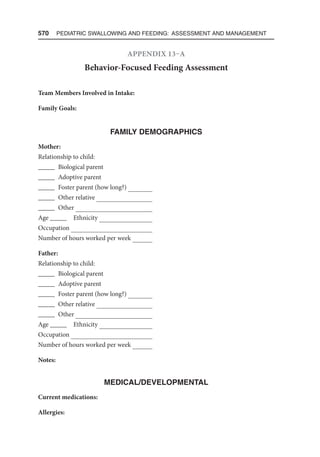































The document is the third edition of 'Pediatric Swallowing and Feeding: Assessment and Management,' which has been updated to reflect advances in understanding the complexities of pediatric swallowing and feeding disorders. It includes contributions from leading experts in the field and emphasizes a multidisciplinary approach to care, addressing genetic factors and the importance of functional assessments. This edition aims to provide essential knowledge for healthcare professionals involved in the management of pediatric feeding and swallowing challenges.










































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

