
Download as PDF, PPTX


![9Copyright © Harvard Business School, 2017
Clinical and Staff Resources Contained within Martini Klinik
Personnel
• Faculty: Urological Surgeons (9)
• Peri-operative staff: nurses (39) [dedicated to prostate cancer]
• Physiotherapists
• Psychologists *
• Oncologists *
• Anesthesiologists *
• Social Workers
• Biostatisticians for clinical trials and outcomes measurement
Facilities
• Operating rooms (4) [dedicated]
• Inpatient ward
• Physiotherapy unit
• Outpatient clinic
• Central Administration and Scheduling
* Employed by Hospital Department but dedicated to Martini Klinik](https://image.slidesharecdn.com/kaplanvbc915-180307170854/85/Robert-Kaplan-Value-Based-Health-Care-9-320.jpg)
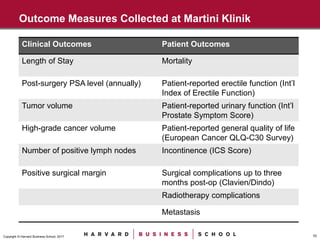
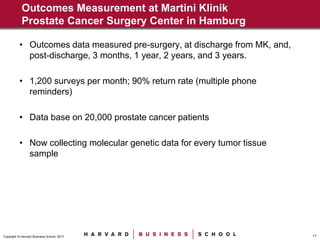

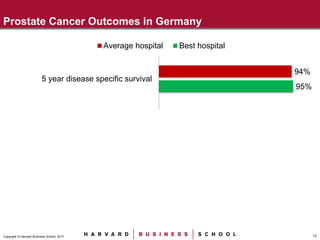
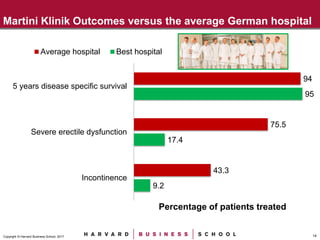
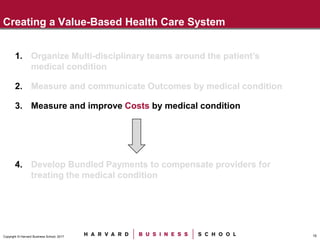
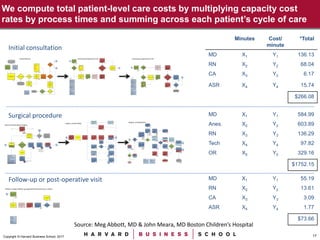

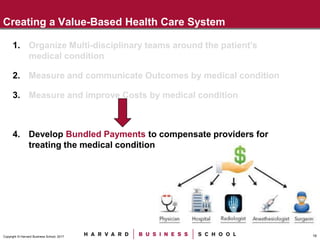
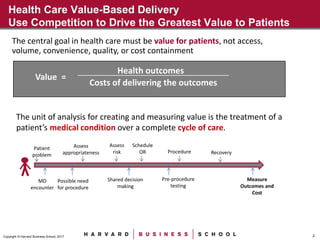
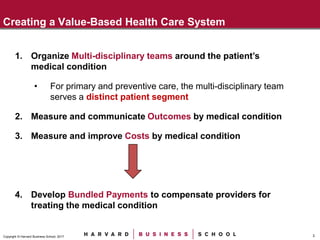
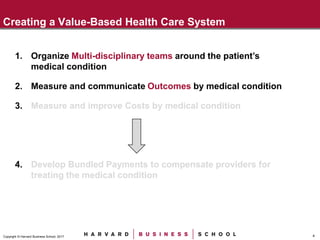
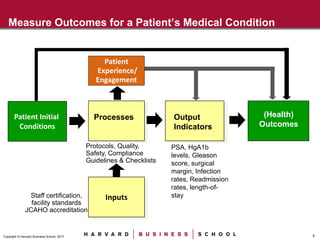
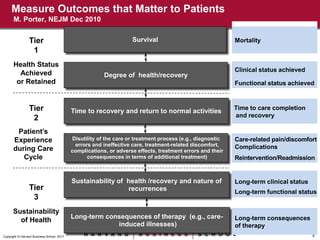
The document discusses creating a value-based healthcare system focused on patient outcomes and costs. It recommends organizing multidisciplinary teams around patient conditions, measuring outcomes and costs by condition, and developing bundled payments to compensate providers for treating a condition over the full cycle of care. The document also provides an example of Martini Klinik in Germany, which achieves better prostate cancer outcomes than average hospitals through dedicated teams, extensive outcomes tracking, and peer comparison.


















































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


