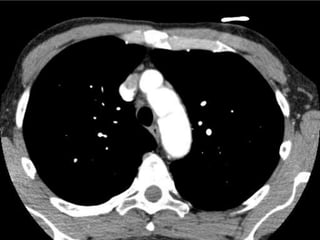
Aortic Dissection 1
•Download as PPTX, PDF•
0 likes•2,398 views
Aortic dissection
Report
Share
Report
Share

Recommended
SMV Gas / Caecal Ischaemia
60 year old male presents with acute abdominal pain and hypotension. CT Abdomen demonstrates gas within the superior mesenteric venous system. Bowel wall intramural gas is seen predominantly in the caecum and filling the ileo-colic vein. No definite arterial thrombosis is demonstrated. The patient proceeded to the operating theatre where the caecum was found to be ischaemic and dusky. A right hemicolectomy was performed and the patient was admitted to ICU post-operatively.
Radiology Case 15
50 year old male with a one month history of intermittent fevers and night sweats with back pain.
Background history of open AAA repair and treated Hodgkin's lymphoma which is now in remission.
his CT Abdomen with intravenous contrast in the arterial phase demonstrates stigmata of aortitis secondary to the development of an aortoenteric fistula. Gas is present in the remnant aneurysm sac following the previous abdominal aortic aneurysm repair. There is associated retroperitoneal lymphadenopathy around the aorta and the process is adherent to the third part of the duodenum, which is presumably the source of gas. This implies that a fistulous connection has developed. Catastrophic haemorrhage into the duodenum is possible.
Incidental finding of a contracted gallbladder containing multiple gallstones, consistent with chronic cholecystitis.
Recommended
SMV Gas / Caecal Ischaemia
60 year old male presents with acute abdominal pain and hypotension. CT Abdomen demonstrates gas within the superior mesenteric venous system. Bowel wall intramural gas is seen predominantly in the caecum and filling the ileo-colic vein. No definite arterial thrombosis is demonstrated. The patient proceeded to the operating theatre where the caecum was found to be ischaemic and dusky. A right hemicolectomy was performed and the patient was admitted to ICU post-operatively.
Radiology Case 15
50 year old male with a one month history of intermittent fevers and night sweats with back pain.
Background history of open AAA repair and treated Hodgkin's lymphoma which is now in remission.
his CT Abdomen with intravenous contrast in the arterial phase demonstrates stigmata of aortitis secondary to the development of an aortoenteric fistula. Gas is present in the remnant aneurysm sac following the previous abdominal aortic aneurysm repair. There is associated retroperitoneal lymphadenopathy around the aorta and the process is adherent to the third part of the duodenum, which is presumably the source of gas. This implies that a fistulous connection has developed. Catastrophic haemorrhage into the duodenum is possible.
Incidental finding of a contracted gallbladder containing multiple gallstones, consistent with chronic cholecystitis.
CTPA
45 year old female presents with a 2 day history of intermittent retrosternal chest pain, dyspnoea and exertional syncope.
She is otherwise normally healthy and does not smoke.
Her regular medications are limited to an oral contraceptive pill and MAO inhibitor (antidepressant). She leads a sedentary lifestyle and her work requires her to be seated for 10 hours every day. No recent long-haul travel or surgery. No personal or family history of venous thromboembolic disease.
Her vital signs in the emergency department are HR 84bpm, BP 62/32mmHg, RR 26 breaths/min, Sats 99% on 15L non-rebreather mask, temperature 36.7 degrees Celsius, GCS 15.
Cool peripheries, distended neck veins. Chest clear. Abdomen soft, non-tender. Calves soft, non-tender.
ECG demonstrates sinus rhythm with a q wave in lead III and T wave inversion in lead III.
D-dimer is 4.
A CT Pulmonary Angiogram is performed which demonstrates multiple, large bilateral pulmonary emboli originating in both the left and right pulmonary arteries and extending into all lobar branches and all segmental branches except the left upper lobe. Additionally, there is bowing of the interventricular septum inferior and contrast reflux into the IVC consistent with right ventricular strain. On the lung windows (not included) there is no consolidation to indicate pulmonary infarction.
CT Abdomen and Pelvis - Case 2
68 year old male presents with a 3 day history of severe
right-sided abdominal pain radiating down into his right scrotum. He has had associated vomiting on 3 occasions and his wife reports that the bedsheets and pillow case were drenched with sweat last night.
On examination, his vitals are: 38.6 degrees, 130bpm, 100/60mmHg, 24 breaths/min, 97% sats on room air. His peripheries are warm and vasodilated. Chest is clear. Abdomen demonstrates localised peritonism in the right lower quadrant. Testes are non-tender.
His urine dipstick is negative for blood, leukocytes or nitrites. Labs demonstrate a white cell count 18 and CRP 280. Renal function is normal.
Blood cultures are collected which quickly grow Clostridium.
A CT Abdomen and Pelvis is performed with IV contrast. Review the scan and identify the primary pathology which explains the patient's presentation.
ANSWER:
There is a small right indirect inguinal hernia containing an
enlarged 9.5mm inflamed appendix with associated fat stranding and minimal fluid. This finding of acute appendicitis contained within an inguinal hernia is consistent with Amyand's hernia. There are no features of small or large bowel obstruction. There is no free fluid or gas within the abdomen. There is no definite intraabdominal lymphadenopathy.
Incidentally, there are numerous other findings in this scan, including cholelithiasis without features of cholecystitis; multiple simple liver cysts; bilateral renal cortical cysts; a large hiatal hernia; a 12mm short-axis elongated lesion in the right para-aortic region posterior to the crus of the diaphragm, which may represent a lymph node. Additionally, there is subcutaneous emphysema involving the lower abdominal wall.
Amyand's hernia is a rare form of inguinal hernia in which the vermiform appendix becomes incarcerated within the hernia. Its incidence is less than 1%. The condition is named after Claudius Amyand, an English surgeon, who is attributed with performing the first successful appendicectomy on a young boy who had appendicitis contained within an inguinal hernia.
CT Abdomen and Pelvis
65 year old female presents with a 2 week history of lower abdominal pain and dysuria.
A CT Abdomen and Pelvis with oral and IV contrast was performed. What is the major pathology present in this study which would explain this patient's symptoms? What is the most likely cause?
The significant abnormality in this scan involves the bladder. There is bladder wall thickening, most marked on the lateral aspect where it measures up to 20mm. Additionally, there is significant perivesical stranding and gas within the bladder lumen and wall. The kidneys are normal in appearance. There is no evidence of diverticular disease involving the adjacent sigmoid colon.
These radiological features are consistent with anaerobic cystitis.
Incidentally, did you note the surgical staple line along the stomach wall?
Cloud Privé, Cloud Public, pourquoi choisir?
Cloud Hybride, le meilleur des deux mondes ? Selon plusieurs études menées par le cabinet McKinsey & Company, les problèmes de sécurité des infrastructures en environnement Cloud public ne doivent plus être un frein à son adoption. D’après les travaux réalisés, la plupart des objections soulevées sont pour la plupart exagérées, voire obsolètes, face aux progrès des fournisseurs de solutions Cloud public notamment sur la conformité ou encore l’authentification. Et si le Cloud privé peut constituer une première étape naturelle pour l’entreprise, c’est sans doute le Cloud hybride qu’il trouvera le plus de flexibilité et de réduction des coûts. Profiter de ressources virtuellement illimités pour répondre à des pics ponctuels, rationaliser son PRA ou encore simplifier les échanges avec les entités externes ne sont que quelque uns des scénarios que nous allons détailler dans cette session.
Phone Us ❤85270-49040❤ #ℂall #gIRLS In Surat By Surat @ℂall @Girls Hotel With...
Phone Us ❤85270-49040❤ #ℂall #gIRLS In Surat By Surat @ℂall @Girls Hotel With 100% Satisfaction
micro teaching on communication m.sc nursing.pdf
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
More Related Content
Viewers also liked
CTPA
45 year old female presents with a 2 day history of intermittent retrosternal chest pain, dyspnoea and exertional syncope.
She is otherwise normally healthy and does not smoke.
Her regular medications are limited to an oral contraceptive pill and MAO inhibitor (antidepressant). She leads a sedentary lifestyle and her work requires her to be seated for 10 hours every day. No recent long-haul travel or surgery. No personal or family history of venous thromboembolic disease.
Her vital signs in the emergency department are HR 84bpm, BP 62/32mmHg, RR 26 breaths/min, Sats 99% on 15L non-rebreather mask, temperature 36.7 degrees Celsius, GCS 15.
Cool peripheries, distended neck veins. Chest clear. Abdomen soft, non-tender. Calves soft, non-tender.
ECG demonstrates sinus rhythm with a q wave in lead III and T wave inversion in lead III.
D-dimer is 4.
A CT Pulmonary Angiogram is performed which demonstrates multiple, large bilateral pulmonary emboli originating in both the left and right pulmonary arteries and extending into all lobar branches and all segmental branches except the left upper lobe. Additionally, there is bowing of the interventricular septum inferior and contrast reflux into the IVC consistent with right ventricular strain. On the lung windows (not included) there is no consolidation to indicate pulmonary infarction.
CT Abdomen and Pelvis - Case 2
68 year old male presents with a 3 day history of severe
right-sided abdominal pain radiating down into his right scrotum. He has had associated vomiting on 3 occasions and his wife reports that the bedsheets and pillow case were drenched with sweat last night.
On examination, his vitals are: 38.6 degrees, 130bpm, 100/60mmHg, 24 breaths/min, 97% sats on room air. His peripheries are warm and vasodilated. Chest is clear. Abdomen demonstrates localised peritonism in the right lower quadrant. Testes are non-tender.
His urine dipstick is negative for blood, leukocytes or nitrites. Labs demonstrate a white cell count 18 and CRP 280. Renal function is normal.
Blood cultures are collected which quickly grow Clostridium.
A CT Abdomen and Pelvis is performed with IV contrast. Review the scan and identify the primary pathology which explains the patient's presentation.
ANSWER:
There is a small right indirect inguinal hernia containing an
enlarged 9.5mm inflamed appendix with associated fat stranding and minimal fluid. This finding of acute appendicitis contained within an inguinal hernia is consistent with Amyand's hernia. There are no features of small or large bowel obstruction. There is no free fluid or gas within the abdomen. There is no definite intraabdominal lymphadenopathy.
Incidentally, there are numerous other findings in this scan, including cholelithiasis without features of cholecystitis; multiple simple liver cysts; bilateral renal cortical cysts; a large hiatal hernia; a 12mm short-axis elongated lesion in the right para-aortic region posterior to the crus of the diaphragm, which may represent a lymph node. Additionally, there is subcutaneous emphysema involving the lower abdominal wall.
Amyand's hernia is a rare form of inguinal hernia in which the vermiform appendix becomes incarcerated within the hernia. Its incidence is less than 1%. The condition is named after Claudius Amyand, an English surgeon, who is attributed with performing the first successful appendicectomy on a young boy who had appendicitis contained within an inguinal hernia.
CT Abdomen and Pelvis
65 year old female presents with a 2 week history of lower abdominal pain and dysuria.
A CT Abdomen and Pelvis with oral and IV contrast was performed. What is the major pathology present in this study which would explain this patient's symptoms? What is the most likely cause?
The significant abnormality in this scan involves the bladder. There is bladder wall thickening, most marked on the lateral aspect where it measures up to 20mm. Additionally, there is significant perivesical stranding and gas within the bladder lumen and wall. The kidneys are normal in appearance. There is no evidence of diverticular disease involving the adjacent sigmoid colon.
These radiological features are consistent with anaerobic cystitis.
Incidentally, did you note the surgical staple line along the stomach wall?
Cloud Privé, Cloud Public, pourquoi choisir?
Cloud Hybride, le meilleur des deux mondes ? Selon plusieurs études menées par le cabinet McKinsey & Company, les problèmes de sécurité des infrastructures en environnement Cloud public ne doivent plus être un frein à son adoption. D’après les travaux réalisés, la plupart des objections soulevées sont pour la plupart exagérées, voire obsolètes, face aux progrès des fournisseurs de solutions Cloud public notamment sur la conformité ou encore l’authentification. Et si le Cloud privé peut constituer une première étape naturelle pour l’entreprise, c’est sans doute le Cloud hybride qu’il trouvera le plus de flexibilité et de réduction des coûts. Profiter de ressources virtuellement illimités pour répondre à des pics ponctuels, rationaliser son PRA ou encore simplifier les échanges avec les entités externes ne sont que quelque uns des scénarios que nous allons détailler dans cette session.
Viewers also liked (19)
Recently uploaded
Phone Us ❤85270-49040❤ #ℂall #gIRLS In Surat By Surat @ℂall @Girls Hotel With...
Phone Us ❤85270-49040❤ #ℂall #gIRLS In Surat By Surat @ℂall @Girls Hotel With 100% Satisfaction
micro teaching on communication m.sc nursing.pdf
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Are There Any Natural Remedies To Treat Syphilis.pdf
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Antiulcer drugs Advance Pharmacology .pptx
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Non-respiratory Functions of the Lungs.pdf
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Charaka Samhita Sutra Sthana 9 Chapter khuddakachatuspadadhyaya
Charaka Samhita Sutra Sthana 9 Chapter khuddakachatuspadadhyaya
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdf
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Physiology of Chemical Sensation of smell.pdf
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Ocular injury ppt Upendra pal optometrist upums saifai etawah
This ppt are composed by upendra pal to provide help future optometrist of india
Recently uploaded (20)
Phone Us ❤85270-49040❤ #ℂall #gIRLS In Surat By Surat @ℂall @Girls Hotel With...
Phone Us ❤85270-49040❤ #ℂall #gIRLS In Surat By Surat @ℂall @Girls Hotel With...
Maxilla, Mandible & Hyoid Bone & Clinical Correlations by Dr. RIG.pptx
Maxilla, Mandible & Hyoid Bone & Clinical Correlations by Dr. RIG.pptx
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Are There Any Natural Remedies To Treat Syphilis.pdf
Are There Any Natural Remedies To Treat Syphilis.pdf
Charaka Samhita Sutra Sthana 9 Chapter khuddakachatuspadadhyaya
Charaka Samhita Sutra Sthana 9 Chapter khuddakachatuspadadhyaya
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...
Ocular injury ppt Upendra pal optometrist upums saifai etawah
Ocular injury ppt Upendra pal optometrist upums saifai etawah