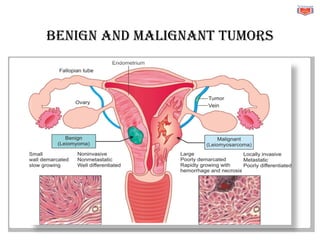
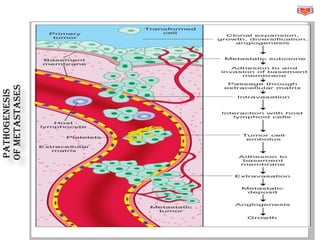
This document provides an overview of cell growth and neoplasms (tumors). It defines a neoplasm and classifies them as benign or malignant tumors. The key differences between benign and malignant tumors are described. Environmental causes of cancer like chemicals, viruses, and radiation are discussed. The document outlines some common clinical features of cancer and laboratory methods to diagnose it, including biopsy, cytology, and genetic testing. It describes dysplasia and carcinoma in situ as premalignant changes. Metastasis, the spread of cancer to other sites, is also summarized. Finally, cancer cachexia, a wasting syndrome common in advanced cancer, is defined.