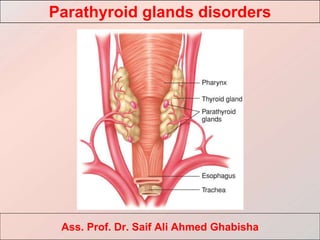
2. Parathyroid glands
• The parathyroid glands (glandulae
parathyreoideae) are represented, as a rule, by
two pairs of small yellow-brown bodies,
closely adjacent to the posterolateral surface
of the thyroid gland, with which they share
innervation and blood supply.
• The upper parathyroid glands are located at
the upper pole of the thyroid gland.
• The lower ones in 20% of cases - in the
anterior mediastinum, are retro-sternal or
ectopic to the stitched-gland, the thymus.
• The size of the parathyroid glands is 5x4x2
mm, the maximum mass is 50 mg.
Parathyroid glands disorders
3. • The main mass of parenchyma of glands consists of the main
parathyroid cells.
• Parathyroid glands (their main and acidophilic cells) produce
parathyroid hormone, which with calcitonin (synthesized by thyroid C-
cells) and vitamin D plays a major role in the regulation of calcium-
phosphorus metabolism.
• Under the action of parathyroid hormone, calcium mobilizes from the
osseous and lacunar bone resorption with the restoration of the level of
calcium in the extracellular fluid.
Parathyroid glands disorders
Physiology-calcium and action of pth action of pth
4. • Bone: enhances resorption of bone matrix by osteoclasts. A prolonged excess
of parathyroid hormone (hyperparathyroidism) leads not only to
demineralization of bone tissue, but also to the destruction of its protein
skeleton (matrix), with hypercalcemia and hypercalciuria.
• Kidney: increases tubular reabsorption of filtered calcium and decreases
tubular reabsorption of filtered phosphate. The action of parathyroid hormone
on the kidneys is to suppress the reabsorption of phosphates in the proximal
sections of the renal tubules, which leads to phosphaturia and
hypophosphatemia, as well as to increase the reabsorption of calcium in the
distal sections of the tubules, i.e., a decrease in urinary calcium excretion.
• Intestine: stimulates renal vitamin D complex synthesis, which increases
intestinal absorption of calcium (indirect effect). In addition, with the
participation of vitamin D, parathyroid hormone increases the reabsorption of
calcium in the intestine.
Parathyroid glands disorders
5. • Parathyroid hormone deficiency (hypoparathyroidism) leads to hypocalcemia,
hyperphosphatemia, and lower levels of calcium and phosphorus in the urine.
Hypersecretion of the hormone causes severe disturbances in mineral
metabolism, and then damage to bones and kidneys.
• It should be remembered that, in addition to parathyroid hormone, calcitonin
and vitamin D, other hormones - glucocorticoids, growth hormone, thyroid
hormones, glucagon, sex hormones, also affect calcium metabolism in the
body.
Parathyroid glands disorders
6. Parathyroid diseases
Hyperparathyroidism
• Hyperparathyroidism is a disease caused by excessive secretion of parathyroid
hormone and characterized by violation of the metabolism of calcium and
phosphorus.
• There are primary, secondary and tertiary hyperparathyroidism.
Parathyroid glands disorders
7. Primary hyperparathyroidism is a pathology of the parathyroid glands
themselves.
Called: adenoma, carcinoma, hyperplasia.
Secondary hyperparathyroidism is a pathology caused by a compensatory
increase in parathyroid hormone production in response to prolonged
hypocalcemia.
Reasons: calcium deficiency in food, chronic renal failure, pathology of the
skeletal system (ostemulation, deforming osteodystorphia), hypovitaminosis D.
Tertiary hyperparathyroidism is a condition that occurs with the development of
an autonomously functioning parathyroid adenoma against the background of a
long-existing secondary hyperparathyroidism.
Parathyroid glands disorders
8. Parathyroid glands disorders
Types of Hyperparathyoidism
Parathyroidectomy for complications
from hypercalcemia.
For adenoma = resect adenoma.
For hyperplasia = resect 31/2 glands or four
glands with autotransplantation.
Intraoperative PTH level should fall by 50%.
Single adenoma (85%) , 4-gland
hyperplasia, carcinoma.
1
Parathyroidectomy for complications.
PO43 binders. Renal transplant. Watch for
calciphylaxis.
Chronic renal failure.
2
Parathyroidectomy if symptomatic or
persistent disease 1 year after
transplant.
Autonomous PTH release after renal
transplant.
3
9. Parathyroid diseases
Hyperparathyroidism
• Primary hyperparathyroidism (Recklinghausen’s disease) is characterized by
an increased content of parathyroid hormone and related lesions of the bone
system, kidneys, stomach and duodenum, pancreas, as well as mental
disorders.
• Primary hyperparathyroidism is caused by solitary adenoma (80–85%), multiple
adenoma (2-3%), hyperplasia (2-12%) or parathyroid cancer (0.5-4.6%).
Parathyroid glands disorders
10. The clinical picture and diagnosis:
• The clinical forms of hyperparathyroidism are: renal, bone, gastrointestinal,
cardiovascular, neuropsychiatric.
• The most common complaints are general weakness, loss of appetite, nausea,
vomiting, constipation, weight loss, pain in bones, muscles, joints, weakness of
limb muscles.
• Often polydipsia, polyuria, a change in the psyche (depression), convulsions,
and a coma join in.
Parathyroid glands disorders
11. Parathyroid glands disorders
Symptoms and signs
system
Polydipsia, weight loss
General
Hypertension, heart block
Cardiovascular
Bone pain, pathological fractures
Musculoskeletal
Anorexia, nausea, constipation
Gastrointestinal
Depression, lethargy, weakness,
psychosis
Neurological
Clinical features of hyperparathyroidism
12. Parathyroid glands disorders
The classic symptoms and signs are:
arthralgia, osteoporosis, and pathologic fractures.
Bones:
renal stones, renal insufficiency, polyuria, and
polydipsia.
Stones:
pancreatitis, peptic ulcer disease, and constipation.
Abdominal groans:
fatigue, weakness, and depression.
Psychic moans:
The clinical picture and diagnosis
13. • In the renal form (30-60%), patients are usually concerned with renal colic,
hematuria, polyuria.
• The disease often proceeds under the mask of urolithiasis.
• Addition of infection and degenerative changes in the kidneys lead to
pyelonephritis, occasionally to nephrocalcinosis, urosepsis and renal failure
(azotemia, uremia).
• The bone form (40-70%) is characterized by pain in the joints, skeletons and
spine.
• Diffuse demineralization of bone tissue is observed.
• Subperiosteal bone resorption is especially characteristic of the phalanges of
the fingers of the hand; osteoporosis of the spine develops.
• As a result of calcium depletion, bones become soft and flexible
(osteomalacia), with curvature and pathological fractures.
Parathyroid glands disorders
The clinical picture and diagnosis
14. • In the gastrointestinal form, a gastric and duodenal ulcer is detected in 15-20%
of patients with primary hyperparathyroidism, which is associated with an
increase in gastrin production as a result of hypercalcemia.
• This leads to hypersecretion of hydrochloric acid and ulceration.
• Peptic ulcer of the stomach can be a manifestation of syndrome MEN I (Wermer
syndrome) - a combination of a tumor (hyperplasia) of the parathyroid glands,
islet-cell tumor of the pancreas and a tumor of the pituitary or MEN IIa.
• In patients with (Wermer syndrome) syndrome, a peptic ulcer often develops
with gastrinomas (Zollinger-Ellison syndrome).
• Chronic pancreatitis (7-15%) is accompanied by the formation of calculi in the
ducts or the deposition of calcium into the pancreatic tissue
(pancreaticalcinosis).
Parathyroid glands disorders
The clinical picture and diagnosis
15. • The diagnosis is made on the basis of an anamnesis (take careful history,
including records or medications, symptoms, prior head and neck radiotherapy,
and other endocrinopathies in the patient and the patient’s family),
• Result given by an X-ray examination of the bones of the hands, skull, long
bones,
• Studies of a biopsy specimen of the iliac bone, conducted to detect
characteristic fibroosteoclasia,
• As well as on the basis of a study of the kidneys, stomach and duodenum,
pancreas,
• Assessment of laboratory parameters (increased levels of parathyroid
hormone, hypercalcemia and hypercalciuria).
• Ultrasound examination (possibly with a puncture biopsy), CT, MRI scans are
performed for the purpose of topical diagnosis and clarification of the
morphological changes of the parathyroid glands.
Parathyroid glands disorders
The clinical picture and diagnosis
16. Treatment:
The only radical method of treatment is surgical.
Indications of surgery
• Age <50 years.
• Older age patients with psychiatric symptoms.
• Life threatening episode of hypercalcemia.
• Presence of renal stones.
• Patient preference.
• Serum calcium elevated >1 mg/dL greater than the higher limit of normal.
• Elevated 24 hour urinary calcium level (>400 mg/day).
• Creatinine clearance reduced by 30%.
• Decreased bone mineral density.
Parathyroid glands disorders
17. Treatment:
• In the preoperative period, phosphates, bisphosphonates are used orally or
intravenously to reduce calcium levels, physiological saline (rehydration) is
added intravenously with sodium sulfate, furosemide.
• With high hypercalcemia (about 4 mmol/ l), therapy is shown, similar to that for
hypercalcemic crisis.
• During the operation, an audit of all parathyroid glands is carried out, the use of
intraoperative ultrasound is advisable.
• Identified adenomas (adenomas) of the parathyroid glands are removed.
• With hyperplasia, 3.5 or all 4 glands are removed with subsequent
autotransplantation of parathyroid tissue into the muscle of the forearm.
Parathyroid glands disorders
20. • Hypercalcemic crisis is an acute life-threatening condition observed in 5% of all
patients with primary hyperparathyroidism.
• It usually develops suddenly (with hypercalcemia of 4 mmol / l or more),
accompanied by nausea, indomitable vomiting, sharp muscle weakness, bone
pain, intense abdominal pain, fever up to 40 ° C, neuropsychiatric disorders
(confusion or sudden excitement, delirium, cramps).
• Symptoms of cardiovascular failure progress, dehydration of the body grows.
Perhaps the appearance of gastrointestinal bleeding, the appearance of
perforated ulcers, acute pancreatitis, etc. (a differential diagnosis with a false
"acute abdomen" is necessary).
Parathyroid glands disorders
21. Treatment:
• Conservative treatment is carried out in order to reduce the level of calcium in
the blood.
• Intensive therapy is used: infusion of solutions to fill the deficit of water and
electrolytes, correction of the acid-base state, treatment of cardiopulmonary
disorders.
• To reduce hypercalcemia, diuretics (furosemide, etc.), forced diuresis,
calcitonin, glucocorticosteroids are used, hemodialysis is performed.
• Surgical treatment - the operation is performed within the next few hours, but
only after lowering the level of calcium in the blood and restoring kidney
function. Mortality is about 20%.
Parathyroid glands disorders
22. Secondary hyperparathyroidism (regulatory) is due to a compensatory increase in
parathyroid hormone production in response to prolonged hypocalcemia.
The cause of hypocalcemia can be:
1) a chronic sharp lack of calcium in food;
2) malabsorption syndrome (for example, with Crohn’s disease, pancreatitis);
3) chronic renal failure (an increase in the content of phosphates in the blood
leads to a decrease in the level of calcium, etc.).
With secondary hyperparathyroidism, hyperplasia develops in all four parathyroid
glands.
Parathyroid glands disorders
Indications for parathyroidectomy with secondary hyperparathyroidism:
• Development of open ulcerative skin lesions from calcinosis or calciphylaxis
• Persistent bone pain or pathologic fractures (renal osteodystrophy)
• Ectopic calcifications
• Intractable pruritus
• Worsening disease with failure of medical management
23. Tertiary hyperparathyroidism Prolonged secondary hyperparathyroidism leads to
autonomous PTH production, which continues even after renal transplantation
replaces the previously deficient renal 1α-hydroxylase conversion step.
The development of pseudohyperparathyroidism occurs in cases of secretion of
the parathyroid hormone or a parathyroid hormone-like protein similar to it by
tumors of other organs - bronchogenic cancer, breast cancer, etc.
Parathyroid glands disorders
24. Hypoparathyroidism
• The disease is caused by insufficiency of parathyroid hormone secretion by the
parathyroid glands, a decrease in calcium reabsorption in the tubules of the
kidneys, and a decrease in calcium absorption in the intestine, resulting in
hypocalcemia.
• In clinical practice, the most common is postoperative hypoparathyroidism due
to accidental or forced removal of the parathyroid glands during thyroidectomy
(0.5–3%), especially when they are localized in the thyroid gland tissue. Less
commonly observed is hypoparathyroidism during radiation therapy,
autoimmune diseases (polyendocrine autoimmune syndromes), due to
congenital absence or underdevelopment of the parathyroid glands, after
operations on the parathyroid glands due to hyperparathyroidism.
Parathyroid glands disorders
25. • In the pathogenesis of the disease, hypocalcemia and hyperphosphatemia play
a key role.
• The clinical picture and diagnosis: Hypoparathyroidism is characterized by low
blood calcium, attacks of painful tonic seizures. Most often, cramps occur in
the muscles of the face (sardonic smile), upper limbs ("obstetrician's arm"),
lower limbs ("horse's foot"). They are accompanied by abdominal pain caused
by a spasm of the muscles of the abdominal wall and smooth muscles of the
intestine. Laryngospasm, bronchospasm with the development of asphyxia
may occur.
Parathyroid glands disorders
26. • In latent tetany, in contrast to obvious, seizures can be caused by the use of
special diagnostic tests: when striking in front of the external auditory meatus,
contraction of the muscles of the face occurs at the exit of the facial nerve
(symptom of the tail); when applying a tourniquet to the shoulder area after 2-3
minutes, cramps of the muscles of the hand are observed (the symptom of
Trousseau is the “obstetrician's arm”); when striking at the outer edge of the
orbit, contraction of the circular muscle of the eyelids and frontal muscle
occurs (Weiss symptom).
Parathyroid glands disorders
27. • Laboratory studies are characterized by a well-known triad - hypocalcemia,
hyperphosphatemia and hypocalceuria.
• Postoperative transient hypocalcemia can be caused by trauma or ischemia of
the parathyroid glands, as well as a sharp increase in calcium absorption by
the bones after eliminating high levels of thyroid hormones during operations
for DTD (the so-called bone hunger). In the case of constant hypocalcemia, the
determination of the level of parathyroid hormone is indicated.
• Treatment: Attacks of tetany are stopped by slow intravenous administration of
a 10% solution of calcium chloride or calcium gluconate. The main role in the
treatment of hypoparathyroidism is assigned to vitamin D2 (calciferol, ergo-
calciferol - 50-100 thousand units / day) and D3 (cholecalciferol) in combination
with calcium preparations (1-2 g / day). Less often, replacement therapy with
parathyroid hormone is performed.
Parathyroid glands disorders
28. Tumors of the parathyroid glands
• Benign tumors of the parathyroid glands (adenomas) and malignant tumors (cancer) are
rare and almost always have hormonal activity, which is an important diagnostic sign.
• Adenomas often develop from the main parathyroid cells and are localized in one of the
lower glands.
• With an increase in the size of several parathyroid glands, a differential diagnosis with
hyperplasia should be made.
• In the clinical picture, the phenomena of hyperparathyroidism come to the fore.
• In topical diagnostics, ultrasound with a thin-needle biopsy, combined radioisotope
research with C20 | T1 and "" Tc, CT and MRI are of great importance.
• In complex diagnostic cases, selective arteriography and selective venous blood
sampling are performed to study parathyroid hormone levels.
• Surgical treatment - removal of adenoma.
Parathyroid glands disorders
29. Cancer:
• Malignant transformation of the parathyroid glands is detected in primary
hyperparathyroidism in 0.5-4.6% of cases.
• The disease occurs with the same frequency in men and women, usually aged
50-60 years.
• A familial form of cancer is described, as well as cancer of the parathyroid
glands in MEN-1 syndrome. (Multiple Endocrine Neoplasia).
• Symptoms of the disease are typical of primary hyperparathyroidism, leading is
severe hypercalcemia.
Parathyroid glands disorders
30. • Hormone-inactive forms are diagnosed extremely rarely (less than 5%).
• The size of the carcinoma is larger than the size of the adenoma.
• Palpable formations on the neck are detected in only 5% of cases.
• Nearly 30% of patients have metastases to the regional lymph nodes of the
neck.
• Sometimes paresis of the recurrent laryngeal nerve develops.
• Distant metastasis occurs mainly in the lungs, less often in the liver and bones.
• The topical diagnosis of the tumor is similar to that of parathyroid adenomas.
Intraoperative ultrasound allows you to evaluate the relationship of the tumor
with surrounding tumors.
Parathyroid glands disorders
31. Surgical treatment:
• Removal of a tumor with an adjacent lobe of the thyroid gland.
• With an increase in regional lymph nodes, lymphadenectomy is performed.
• During surgery, rupture of the capsule of the tumor should be avoided in order
to prevent implantation relapse.
• Local relapses are often observed - up to 50%.
• The morphological diagnosis is difficult to establish even for an experienced
pathologist.
Parathyroid glands disorders
32. Multiple endocrine neoplasia syndromes
Neoplasms can develop synchronously or metachronously
Autosomal dominant, 100% penetrance, variable expressivity
MEN I
Parathyroid hyperplasia
• Usually the first part to become symptomatic; urinary symptoms
• Tx: 4-gland resection with autotransplantation
Pancreatic islet cell tumors
• Gastrinoma
• 50% multiple, 50% malignant – major morbidity of syndrome
Pituitary adenoma
• Prolactinoma
• Need to correct hyperparathyroidism 1st.
Parathyroid glands disorders
33. Multiple endocrine neoplasia syndromes
MEN IIa
Parathyroid hyperplasia (Pheochromocytoma)
• Very often bilateral, nearly always benign
Medullary CA of thyroid
• Nearly all patients; diarrhea most common symptom; often bilateral
• cause of death in these patients
• Usually 1st part to be symptomatic
• Need to correct pheochromocytoma 1st.
Parathyroid glands disorders