1) Paraphilias refer to recurrent and intense sexual urges, fantasies or behaviors that involve unusual objects, activities, or situations and cause distress or impairment. They have been categorized and defined in various ways across different editions of the DSM and ICD classification systems.
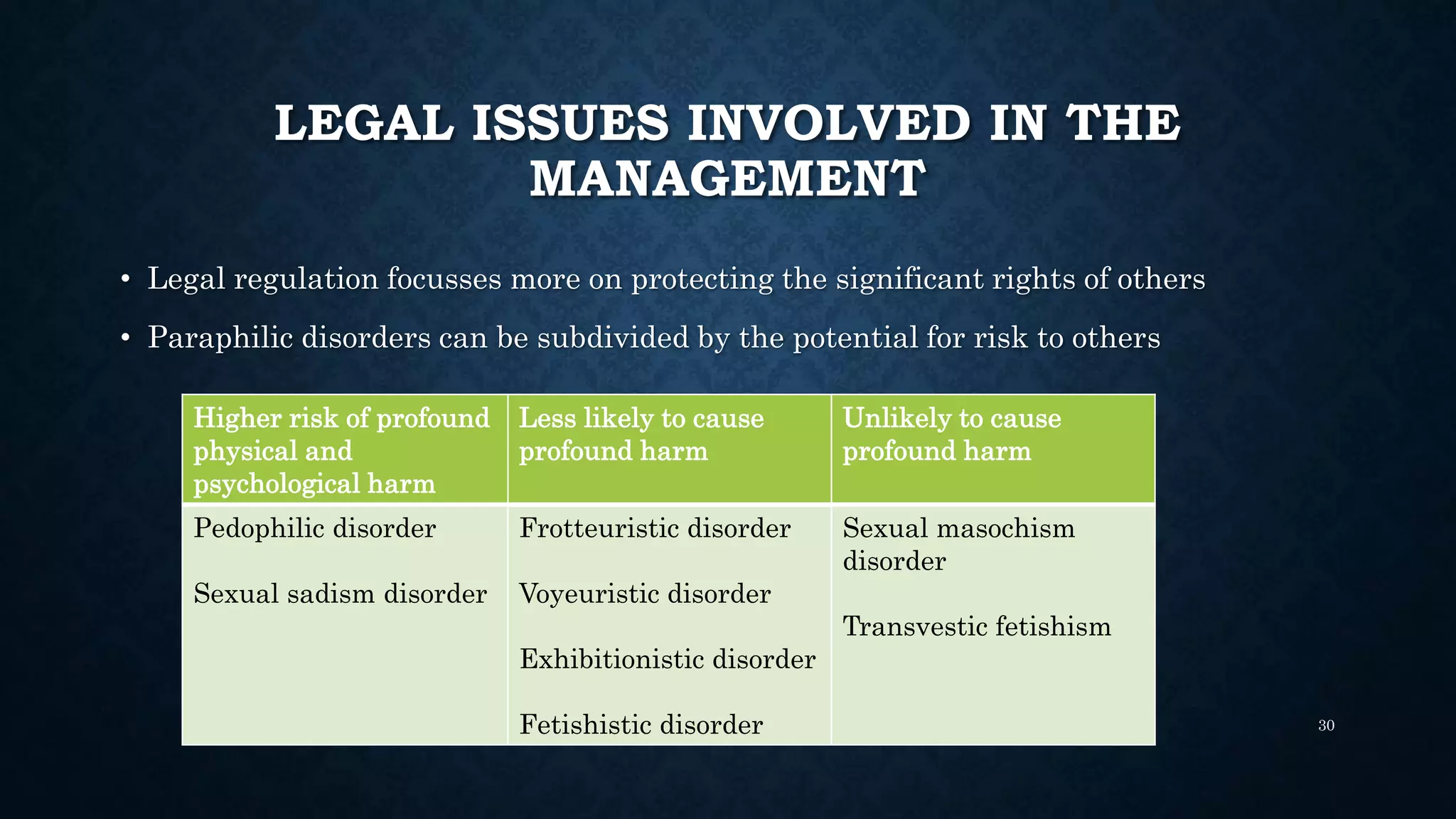
2) Common paraphilic disorders include voyeuristic disorder, exhibitionistic disorder, frotteurism, sexual masochism disorder, sexual sadism disorder, pedophilic disorder, fetishistic disorder, and transvestic disorder.
3) The etiology of paraphilias is complex and multifactorial, involving possible genetic, neurological, environmental, and psychosocial factors. Common comorbidities include other













































































![paraphilias and gender identity [Autosaved] - Copy (2)-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/paraphiliasandgenderidentityautosaved-copy2-1-241003045156-2ba8163c-thumbnail.jpg?width=640&height=640&fit=bounds)




























