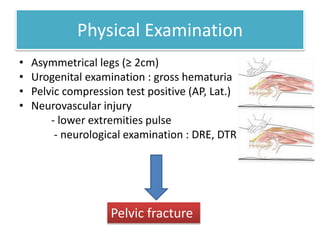
A 30-year-old Thai man was brought to the emergency room 15 minutes after a motor vehicle accident. He was unresponsive with a blood pressure of 80/50 mmHg and pulse of 120/min. A pelvic compression test was positive and his right leg was 3 cm shorter. Initial management included resuscitation with Ringer's lactate and oxygen, monitoring of vital signs, and pain control. Imaging found a fracture of the right pubic rami and left sacrum. The pelvic fracture was classified as Type B or C, indicating rotational and vertical instability. Management included immobilization with a pelvic binder and potential open reduction and internal fixation surgery.





![46 current evidence about femoral neck fracture treatment[1]](https://cdn.slidesharecdn.com/ss_thumbnails/46currentevidenceaboutfemoralneckfracturetreatment1-130613033628-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










































