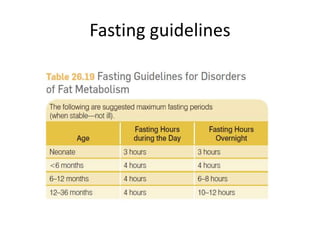
This document discusses nutrition therapy for disorders of fat metabolism. Acute treatment aims to stop catabolism and provides intravenous dextrose and carnitine. Chronic intervention focuses on preventing fasting, limiting fatty acids, and providing alternate substrates like medium-chain triglycerides. Specific disorders require restricted fat intake, with long-chain 3-hydroxyacyl-CoA dehydrogenase deficiency the most restrictive at 25-30% of calories and medium-chain acyl-CoA dehydrogenase deficiency treated by avoiding fasting with feedings every 3 hours.