INTRODUCTION
• According toWHO 2019 report,there are 10
million incident cases of TB in 2018, of which
1.1 million (11 percent) occurred among
children <15 years; similar numbers of boys
and girls were affected.
• In 2019, 2,05,000 deaths occurred due to TB
in children <15 years (32,000 occurring in HIV-
infected children) .
3.
Introduction
• Children upto14 years (35% of Population) –
form 10% of case load.
• Childhood TB is a formidable problem of which
pulmonary TB most common.
• Extra Pulmonary TB is more common in adults.
• Adults and older children have an infectious
from of TB and is more easily diagnosable due
to their capacity to bring up sputum.
4.
NATIONAL TB CONTROLPROGRAMME
• The National TB Programme (NTP) was launched by
the Government of India in 1962 in the form of
District TB Centre model involved with BCG
vaccination and TB treatment.
• The Government of India revitalized NTP as Revised
National TB Control Programme (RNTCP) in the same
year. DOTS was officially launched as the RNTCP
strategy in 1997 and by the end of 2005 the entire
country was covered under the programme.
• During 2006–11, in its second phase RNTCP
improved the quality and reach of services, and
worked to reach global case detection and cure
targets.
5.
• National StrategicPlan for Tuberculosis Control
2012-2017 was documented with the goal of
‘universal access to quality TB diagnosis and
treatment for all TB patients in the community’.
• Renaming of RNTCP
• Union government changed the name of Revised
National Tuberculosis Control Program (RNTCP)
to National Tuberculosis Elimination Program
(NTEP) in December 2019, as declared by Special
Secretary, Ministry of Health and Family Welfare,
in a letter to all the State Chief Secretaries.
6.
National strategic planfor tuberculosis
elimination 2017-2025
• RNTCP has released a ‘National strategic plan for
tuberculosis 2017-2025’ (NSP) for the control and
elimination of TB in India by 2025. According to the
NSP TB elimination have been integrated into the
four strategic pillars of “Detect – Treat – Prevent –
Build” (DTPB).
• Detect:
• Notification of TB cases
• NIKSHAY: To facilitate TB notification, RNTCP has
developed a case-based web-based TB surveillance
system called “NIKSHAY” (https://nikshay.gov.in ) for
both government and private health care facilities.
7.
• Public privatepartnership
The incentives to the Private Sector TB Care Provider
are as follows:
• Rs 250/- on notification of a TB case diagnosed as per
Standards for TB Care in India (STCI)
• Rs 250/- on completion of every month of treatment
• Rs 500/- on completion of entire course of TB treatment
• Rs 2750/ for notification and management of a drug-
sensitive patient over 6-9 months as per STCI
• Rs 6750/-for notification and correct management of a
drug-resistant case over 24 months as per STCI
• Free drugs and diagnostic tests to TB patients in private
sector
8.
• Treat:
• FDCs
• Nikshya poshak yojana: It is centrally
sponsored scheme under National Health
Mission (NHM)
• Financial incentive of Rs.500/- per month is
provided for nutritional support to each
notified TB patient for duration for which the
patient is on anti-TB treatment.
• Incentives are delivered through Direct benefit
transfer (DBT) scheme to bank accounts of
beneficiary.
9.
• Expending optionsfor ICT based treatment adherence
support mechanisms:
• Mobile based “Pill-in-Hand” adherence monitoring tool
• Interactive Voice Response (IVR), SMS reminders.
• Specially designed electronic pill boxes or strips with
GSM connection and pressure sensor
• Patient Compliance toolkit: a mobile app for patients to
report treatment compliance using video, audio or text
message
• Automated pill loading system
• Innovatively designed ICT enabled smart cards SMS
gateway
10.
• Intensifying TBcontrol activities in following key populations is
addressed in NSP:
• TB-HIV
• Diabetics, Tobacco use and Alcohol dependence
• Poor, undernourished, economically and socially backward
communities
• TB control in hilly and difficult terrains
• Substance dependence and sexual minorities
• TB and pregnancy
• Paediatric population
• Prison Inmates and staff of prisons/jails
• management of extra pulmonary TB
• Prevent:
• Air borne infection control measures
• Contact tracing
• Isoniazid Preventive Therapy (IPT)
11.
• Isoniazid PreventiveTherapy (IPT)
• Recommended to Children < 6 years of age, who are
close contacts of a TB patient. Children will be
evaluated for active TB by a medical officer/
pediatrician and after excluding active TB he/she will
be given INH preventive therapy.
• Also given to all HIV infected children who either had
a known exposure to an infectious TB case or are
Tuberculin skin test (TST) positive (>=5mm
induration) but have no active TB disease.
• All TST positive children who are receiving
immunosuppressive therapy (e.g. Children with
nephrotic syndrome, acute leukemia, etc.).
12.
• A childborn to mother who was diagnosed to have TB in
pregnancy will receive prophylaxis for 6 months, provided
congenital TB has been ruled out. BCG vaccination can be
given at birth even if INH preventive therapy is planned.
• Close contacts of index cases with proven DR-TB (drug
resistant-TB) will be monitored closely for signs and
symptoms of active TB as isoniazid may not be prophylactic
in these cases.
• BCG vaccination- It is provided at birth or as early as
possible till one year of age. BCG vaccine has a protective
effect against meningitis and disseminated TB in children.
• Addressing social determinants of TB like poverty,
malnutrition, urbanization, indoor air pollution, etc. require
inter departmental/ ministerial coordinated activities and
the programme is proactively facilitating this coordination.
13.
• Build:
• NSP2017-2025 is recommends strengthening
health system in the form of building and
enabling policies, empowering institutions and
human resources with enhanced capacities.
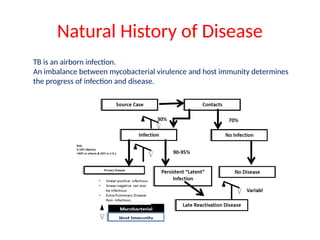
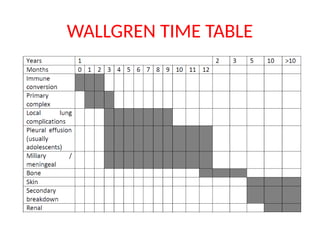
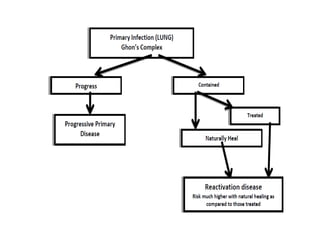
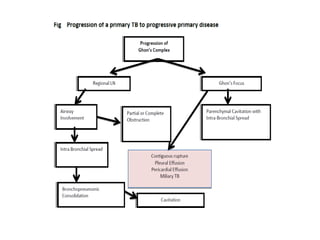
Natural History ofDisease
TB is an airborn infection.
An imbalance between mycobacterial virulence and host immunity determines
the progress of infection and disease.
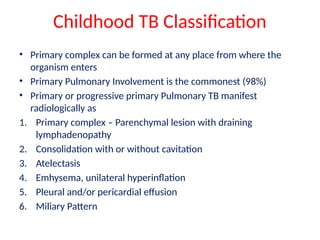
Childhood TB Classification
•Primary complex can be formed at any place from where the
organism enters
• Primary Pulmonary Involvement is the commonest (98%)
• Primary or progressive primary Pulmonary TB manifest
radiologically as
1. Primary complex – Parenchymal lesion with draining
lymphadenopathy
2. Consolidation with or without cavitation
3. Atelectasis
4. Emhysema, unilateral hyperinflation
5. Pleural and/or pericardial effusion
6. Miliary Pattern
20.
Reactivation or Postprimary TB
It is a disease of adolosence and adulthood
• 50-90% result from reactivation of previously
dormant infection
• Prediliction for apical or posterior segement of
upper lobes or superior segement of lower
lobes
• Usually appears as focal or patchy
consolidation, consolidation with cavitation
and pleural extension
21.
CASE DEFINITIONS TB
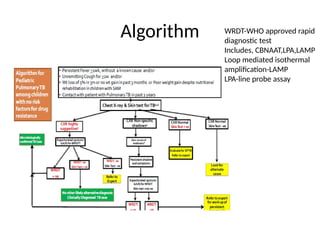
•Presumptive pediatric TB :- refers to children with
persistent fever and / or cough for more than 2 weeks, loss
of weight/ no weight gain and / or history of contact with
infectious TB cases
• History of unexplained weight loss or no weight gain in
past 3 months
• loss of weight is defined as loss of weight of more than 5
% body weight as compared to highest body weight
recorded in last 3 months.
• In a symptomatic child contact with a person with any form
of active TB within last 2 years may be significant
22.
• Presumptive extrapulmonary TB
• Refers to a presence of organ specific symptoms and signs like
swelling of lymph nodes, pain and swelling in joints, neck
stiffness, disorientation etc. and or/ constitutional symptoms
like significant weight loss, night sweats, persistent fever >=2
weeks.
• Presumptive DR TB
• Referred to those TB patients who have failed treatment with
first line Drugs, pediatric TB non responders, TB patients who
are in contact with DR-TB.
• TB patients who are positive on any follow up sputum smear
examination during treatment with first line drugs
• Previously treated TB cases and TB patient with HIV co-
infection
23.
DIAGNOSIS OF TB- CHILDREN
• In children with presumptive pediatric TB every attempt
should be made to microbiologically prove diagnosis.
• If M. Tuberculosis is not detected or specimen is not
available, diagnosis is inferred from Chest X-Ray (CXR) and
Tuberculin Skin Test (TST) by Mantoux technique using 2 TU
of PPD RT23.
CB NAAT ( Catridge Based Nucleic Acid amplification Test )
• Game Changer ( Higher sensitivity than smear )
• But fails to pick nearly 50% of the cases
• CB NAAT best yield -- when ordered on basis of positive chest
skiagram than chest symptoms
• Diagnosis is based on combination of indirect clues,
symptomatology, radiology, contact history, positive TST.
• All children with TB should be offered HIV testing
Bacteriological diagnosis:
• Bacteriologicaldiagnosis includes microbiological
diagnosis (smear/cultures) and molecular diagnosis
(CBNAAT).
• Bacteriological diagnosis is the only confirmatory
method of diagnosis of TB
• Early morning gastric aspirate is a preferred specimen
for most young children with presumptive TB. It needs
overnight fasting; requires hospitalization and skilled
staff. It requires centrifugation.
• Induced sputum is another sample which can be
obtained in children who are unable to produce
sputum.
26.
• CBNAAT isa real-time PCR rapid technique for diagnosis of TB and
detection of rifampicin-resistance conferring mutations within 2
hours.
• CBNAAT can be performed on both respiratory and non-respiratory
specimens (GA, BAL, IS, pleural fluid, CSF, lymph node aspirate etc).
• CBNAAT is now recommended in all children for diagnosis of TB
• A new paediatric TB case, diagnosed by upfront CBNAAT, without
any risk factor for DRTB is currently retested with a fresh specimen.
• If the repeat sample is also showing Rifampicin resistance, then the
case is classified as ‘MDR Case’.
• As a gold standard for diagnosis and for phenotypic DST, currently
liquid cultures like Mycobacterium Growth Indicator tube™ (MGIT)
cultures are used and recommended..
• Cultures should be sent in all children who are CBNAAT negative
and all presumptive DR TB
27.
• Diagnosis ofExtra pulmonary TB (EPTB)
• EPTB refers to any microbiologically confirmed or
clinically diagnosed case of TB involving organs
other than lungs e.g. lymph nodes, pleura, bones,
joints, intestine, genitourinary tract, meninges of
the brain etc.
• CBNAAT is preferred over other tests.
• Sensitivity of CBNAAT for TB is high in FNAC/biopsy
specimen from lymph nodes/ other tissues and CSF
but lower in pericardial, ascetic & synovial fluid
samples and still lower in pleural fluid
28.
• TB lymphadenitis
•Lymph node TB is one of the most common forms of EPTB
and cervical lymph nodes are the most common site with
or without associated disease of other lymphoid tissue.
• It usually occurs in 5-9 years of age.
• Clinical correlate of diagnosis includes progressive
enlargement of lymph node for more than 2 weeks, firm,
minimally tender or non-tender, with or without
fluctuation, further may get matted and develop chronic
sinus formation.
• Fine needle aspiration cytology (FNAC) is usually
adequate for accurate diagnosis and it correlates well
with biopsy in more than 90% of cases.
• Histopathology, typically shows necrosis and epithelioid
granuloma.
29.
TB meningitis
• CSFis mostly clear, leucocyte counts ranges from 10 to
500 cells /mm3 (occasionally higher), and majority are
lymphocytes, glucose usually remains below 40mg/dl
(CSF glucose / blood glucose below 0.5, protein is
elevated (more than 100 mg/dl).
• Tuberculin Skin Test may be not reactive in 50% cases
• CECT heads is the initial modality of diagnosis
• Contrast MRI has higher sensitivity than CECT for
abnormalities such as meningeal
enhancements ,infarcts,tuberculomas and lesions
involving brain stem.
30.
• Bone andJoint TB
• Bone and Joint TB roughly accounts for 5-15% of
all EPTB and 2-5% of all TB in children and adults.
• Symptomatic disease usually develops within 1-
3years of infection but TB dactylitis can have an
early manifestation (usually 1month).
• Common presentations of Bone and Joint TB are
Potts spine (50% of osteoarticular TB), Dactylitis,
Arthritis (as extension from the metaphysitis),
Osteomyelitis. A few uncommon ones are reactive
arthritis (Poncets), tenosynovitis and bursitis.
31.
• Potts spine
•Most common site of Potts Spine is thoracic, followed by
lumbar/ cervical. Pain may be localized over the involved
vertebra or could be referred due to root pains
• There can be local tenderness or deformity. Fever and
constitutional symptoms present in one among three cases
• Neurological complications include paraparesis in 20-50%
cases, cauda equina syndrome, 15% of patients have a
paradoxical response with increased neurologic deficit
following therapy
• A risk of kyphosis later in life; especially in children below
7-10 years.
• MRI is the most sensitive (nearly 100%).
32.
TREATMENT OF TUBERCULOSIS
•Isoniazid (INH) and rifampicin (RMP) kill the fast-growing bacilli
• Pyrazinamide (PZA) acts against intracellular organisms in
acidic medium
• Extracellular slow growing bacilli are best killed by RMP.
• EVERY CASE OF TUBERCULOSIS MUST BE TREATED AT LEAST
WITH THESE DRUGS.
• Ethambutol is recommended as fourth drug in intensive phase
and as a third drug in the continuation phase due to high INH
resistance (around 13%) in new cases.
WHY DAILY THERAPY?
• Longer duration of rifampicin treatment,
• Daily therapy early in the treatment
• Regimens that included a greater number of drugs
Lower relapse, failure, and acquired drug resistance rates
33.
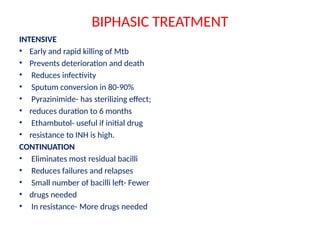
BIPHASIC TREATMENT
INTENSIVE
• Earlyand rapid killing of Mtb
• Prevents deterioration and death
• Reduces infectivity
• Sputum conversion in 80-90%
• Pyrazinimide- has sterilizing effect;
• reduces duration to 6 months
• Ethambutol- useful if initial drug
• resistance to INH is high.
CONTINUATION
• Eliminates most residual bacilli
• Reduces failures and relapses
• Small number of bacilli left- Fewer
• drugs needed
• In resistance- More drugs needed
34.
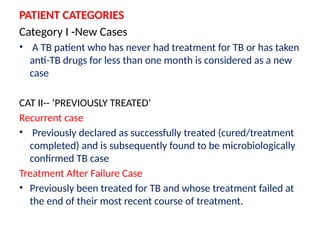
PATIENT CATEGORIES
Category I-New Cases
• A TB patient who has never had treatment for TB or has taken
anti-TB drugs for less than one month is considered as a new
case
CAT II-- ‘PREVIOUSLY TREATED’
Recurrent case
• Previously declared as successfully treated (cured/treatment
completed) and is subsequently found to be microbiologically
confirmed TB case
Treatment After Failure Case
• Previously been treated for TB and whose treatment failed at
the end of their most recent course of treatment.
35.
• CAT II-‘PREVIOUSLY TREATED’ CTD…
Treatment After Lost to Follow Up Case
• Previously treated for TB for 1 month or more and
was declared lost to follow up in their most recent
course of treatment and subsequently found
microbiologically confirmed TB case
Other Previously Treated Case
• Those who have previously been treated for TB
but without outcome after their most recent
course of treatment is unknown or undocumented
FIXED DOSE COMBINATIONS(FDC)
• Safety
• Simplified treatment
• No errors in missing one or more of the
combination drugs
• Reduced risk of emergence of drug-
resistant strains
• Programmatic view point- Simplify drug
supply management, shipping and
distribution
39.
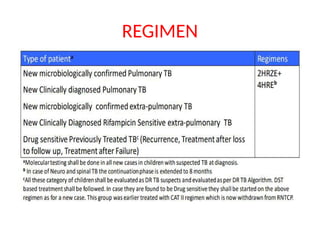
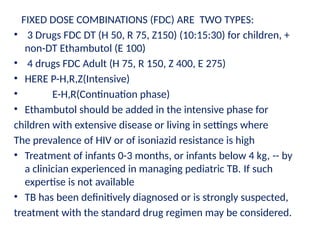
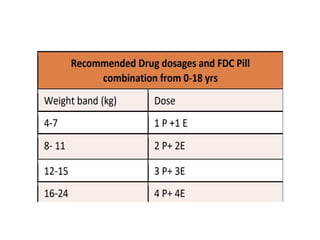
FIXED DOSE COMBINATIONS(FDC) ARE TWO TYPES:
• 3 Drugs FDC DT (H 50, R 75, Z150) (10:15:30) for children, +
non-DT Ethambutol (E 100)
• 4 drugs FDC Adult (H 75, R 150, Z 400, E 275)
• HERE P-H,R,Z(Intensive)
• E-H,R(Continuation phase)
• Ethambutol should be added in the intensive phase for
children with extensive disease or living in settings where
The prevalence of HIV or of isoniazid resistance is high
• Treatment of infants 0-3 months, or infants below 4 kg, -- by
a clinician experienced in managing pediatric TB. If such
expertise is not available
• TB has been definitively diagnosed or is strongly suspected,
treatment with the standard drug regimen may be considered.
42.
• ADJUNCT STEROIDS-DEFINITE INDICATIONS
• TB meningitis, pericarditis, addison disease, miliary TB with
alveolo-capillary block and TB uveitis
• Steroids may be used in -Endobronchial tuberculosis,
Bronchial compression, mediastinal compression syndrome,
Pleurisy with severe distress, laryngeal TB,TB IRIS
• Evidence in other forms of intracranial TB like tuberculomas
is unclear.
• Tuberculosis-immune reconstitution inflammatory
syndrome is an excessive immune response
against Mycobacterium tuberculosis that may
occur in either HIV-infected or uninfected patients,
during or after completion of anti-TB therapy.
43.
Adjunct- steroids:
• Predinsolone1-2 mg/kg/day (or)
• Dexamethasone 0.6 mg/kg/day (or)
• Equivalent steroid is used for 4 weeks and then tapered over
next 4 weeks
• Pyridoxine supplementation -current recommendation:
Pyridoxine 10mg per day
Justification for recommendation:
• Increased INH dose to 10-15 mg/kg for treatment and
prophylaxis and it can potentially increase the dose related
adverse effects.
• High prevalence of malnutrition in children with TB.
• Difficult to diagnose peripheral neuropathy in young children
(if unrecognised, may result in severe & prolonged morbidity)
44.
MONITORING AND FOLLOW-UP
1.Clinical follow-up
2. Laboratory follow-up
CLINICAL FOLLOW-UP
• Frequency of visits:
• Initial visit within 2 weeks of starting therapy (to check dose/ combination/
tolerance)-where possible
• Every month during treatment
• Every 6 months for 2 years (after completion of treatment)
• Improvement in clinical symptoms
• Physical examination
• Side effects of medications
• Treatment of Co-morbid conditions
• Adherence to therapy
• Use Pill count, Social support, family based DOT and Treatment supervisor as
needed
• In case the patient has interrupted treatment:
• Interruption upto 4 weeks- Resuming the therapy
• Interruption for over 4 weeks- Investigated for acquisition of DRTB
45.
MONITORING AND FOLLOW-UPLAB INVESTIGATIONS
• Microbiological: At end of IP and end of
treatment(Bacterial negativity- sputum, GA etc with
smear and culture; repeat CBNAAT for any acquisition
of Rif Resistance if follow-up smear is positive)
• MGIT culture: should be performed if child is not
responding even after 4 weeks of therapy.
• Liver function tests:No routine LFT for patients on first
line drugs.
• Followup chest radiographs:
• Usually done at the end of therapy
• Earlier if no clinical improvement,complications or
deterioration.
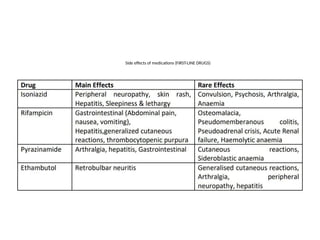
• SIDE EFFECTSOF MEDICATIONS----ATT
INDUCED LIVER INJURY
• Definition:
• Presence of at least rise of >5 times the upper
limit of normal levels of ALT and /or AST, even
when has no symptoms or
• rise in ALT (and/or) AST >3 times with nausea,
vomiting, diarrhoea or rise in level of serum
total bilirubin above 1.5 mg/dl.
• Usually within weeks to months (60% in the
first 3 months)
48.
ATT INDUCED LIVERINJURY--MANAGEMENT
• If injury fulfills criteria
• Stop all hepatotoxic ATT drugs - R, H, Z immediately
• Symptomatic treatment should be given.
• Look for other causes of hepatitis- viral markers in all cases (A,
E).
• Consider starting alternative drugs if seriously ill: Ethambutol,
Streptomycin, &Levofloxacin.
• Reintroduce primary drugs once symptoms subsided & liver
enzymes < 2ULN. The drugs (in full dose) are to be added
every 3-days, with regular LFT monitoring.
49.
• A newdrug is re-instituted only if the ALT is
less than twice the upper limit of normal.
• In case the patient is sick, drowsy or have any
abnormal bleeds, the case should be referred
to an in-patient facility.
• For deciding the final duration of therapy; do
not take into account the days when full
complement of treatment was not given
50.
Drug Resistant TBincluding MDR
• MDR-TB is defined as M. tuberculosis resistant
to isoniazid and rifampicin with or without
resistance to other drugs. Currently, WHO
estimated incidence of Rifampicin and MDR TB
in India is estimated to be around 147000
translates to be around 11 patients per 100 000
population annually as per the Global TB
Report, WHO 2017
• MDR TB in children mirrors MDR TB in adult so
MDR TB is common in children in settings
where MDR TB is common in adults.
51.
• Presumptive caseof MDR-TB in children- Children
who are contacts of adults with MDR TB/drug
resistant TB, who are lost to follow up after
initiating treatment, those who present with
recurrence of disease after previous treatment,
those who do not respond to therapy with first line
drugs and those living with HIV
• Bacteriological confirmation and drug susceptibility
testing are mandatory.
• sputum must be collected in all children with
presumed DR-TB for CB NAAT (e.g. Xpert MTB/RIF)
or LPA AND culture and drug sensitivity testing
52.
• Probable MDR-TB:children wherein bacteriologic
confirmation is not available/ negative and the
decision regarding diagnosis and initiation of
treatment is taken by the NDR-TBC committee. They
include children who have:
➢ Close contact with a known case of MDR-TB;
➢ Close contact with a person who died whilst on TB
treatment;
➢ Close contact with a person who failed TB treatment;
➢ Non response or Failure of a first-line regimen,
recognizing that both bacteriological and Clinical
definitions of failure should be used; and
➢ Previous treatment with second-line medications
53.
• ‘A patientis confirmed to have drug resistant TB,
only when the results are from a RNTCP quality
assured Culture & DST Laboratory and by a RNTCP
endorsed testing method’
• Mono-resistance TB (MR)- A TB patient, whose
biological specimen is resistant to one firstline Anti-
TB drug only
• Poly-drug resistance TB (PDR)-A TB patient, whose
biological specimen is resistant to more than one
first-line anti-TB drugs, other than both H & R.
54.
• Rifampicin resistance(RR)- A TB patient, whose biological
specimen is resistant to R, detected using phenotypic or
genotypic methods, with or without resistance to other
anti-TB drugs. It includes any resistance to R, in the form of
mono-resistance, poly-resistance, MDR or XDR.
• Multidrug resistance TB (MDR)- A TB patient whose
biological specimen is resistant to both H & R with or
without resistance to other first-line anti-TB drugs. MDR TB
patients may also have additional resistance to any/all FQ
OR any/all SLI anti-TB drugs.
• Extensive drug resistance (XDR)- A MDR TB patient whose
biological specimen is additionally resistant to at least a FQ
(Ofx, Lfx, Mfx) and SLI anti-TB drugs (Km, Am, Cm).
• It is to be noted that R resistance is quite rare without H
resistance.
55.
• Choice ofDiagnostic Technology
• CBNAAT/LPA--- First
• Liquid culture isolation and LPA DST--- Second
• Liquid culture isolation and liquid DST ---Third
56.
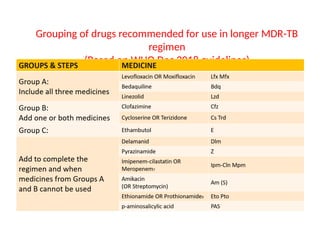
Grouping of drugsrecommended for use in longer MDR-TB
regimen
(Based on WHO Dec 2018 guidelines)



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






