Download to read offline

![1112 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
insights into progressive and subtle neurological changes associated with dietary factors in individuals at risk for or living with
AD. In addition, greater understanding of mechanisms involved in nutritional influences on AD risk and progression, such as
oxidative stress and loss of neuronal membrane integrity, will better inform possible interventional strategies. There is consensus
among the authors that nutritional deficits, and even states of excess, are associated with AD, but more work is needed to
determine cause and effect. Appropriately designed diets or nutritional interventions may play a role, but additional research is
needed on their clinical–cognitive effectiveness.
Keywords: Alzheimer’s disease, cognition disorders, diet therapy, neuronal membrane, nutrition
INTRODUCTION
Alzheimer’s disease (AD) has a complex, multi-
factorial pathophysiology involving amyloid plaques,
neurofibrillary tangles, and decreased number of
synapses [1]. A broad range of studies, from preclin-
ical to epidemiological, point to an important role
for diet and nutritional status in AD (reviewed in
[2, 3]). While AD is not the result of a single spe-
cific nutrient deficiency, accumulating evidence shows
that nutritional factors can influence both the risk of
developing AD and subsequently its rate of clinical
progression [2, 4]. As a result, dietary and lifestyle
guidelines have been proposed to help adults reduce
their risk [5]. However, further evidence is required to
demonstrate that modification of an individual’s nutri-
tional status can protect the brain and prevent, delay,
or reduce the pathophysiological consequences of AD
[6]. With this challenge in mind, the authors convened a
roundtable discussion, with support provided by Nutri-
cia, to examine the role of nutrition in AD and to
discuss proposals for raising awareness of nutrition as
an important topic for future research projects in AD.
Indeed, the authors have formed a new Professional
InterestArea(PIA)withintheAlzheimer’sAssociation
Society to Advance Alzheimer’s Research (ISTAART)
to improve the quality of studies in this field. This paper
summarizes the proceedings from the roundtable meet-
ing and includes a synopsis of individual presentations
together with a summary of the roundtable discussion.
OVERWEIGHT, OBESITY, AND THE BODY
WEIGHT LOSS TRAJECTORY IN AD
Deborah Gustafson
Some epidemiological studies show that being over-
weight or obese in midlife, measured as body mass
index (BMI) or central adiposity (waist circumference
or waist-to-hip ratio), may increase the risk of AD
and other dementias decades later, although conflict-
ing results have been reported [7–11]. Studies using
traditional anthropometric cut-points for BMI, waist
circumference, and waist-to-hip ratio have shown that
in adult midlife (reported as approximately mid-30 s to
60 years), being overweight or obese increases the risk
of late-onset dementia [12]. However, after midlife,
these anthropometric measures of body weight and
BMI tend to decrease and subsequently higher levels of
body weight, BMI, and/or overweight and obesity are
associated with a lower risk of dementia. Data suggest
that individuals who are underweight and/or experi-
ence a decrease in BMI in late-life have a higher risk
of dementia than individuals whose BMI is in the nor-
mal range or stable [8, 13]. In addition to increasing
the risks of developing dementia and AD, being over-
weight or obese is associated with cognitive decline,
brain atrophy, white matter changes, and disturbances
of blood-brain barrier integrity [9, 12, 13]. There is
one study of two million people suggesting that under-
weight measured at any time from age 40 years and
older, is a risk factor for dementia [11]. Given the
observed trajectory of BMI over the life course and
in relation to dementia described below, these data are
difficult to interpret.
The association between adiposity and dementia is
complicated by the natural BMI trajectory over an indi-
vidual’s life course [8]. In a longitudinal study among
Swedish women followed over 37 years, BMI trajec-
tories as a function of age differed between women
who did versus those who did not develop demen-
tia. There was a smaller increase in BMI from age 38
to 70 years in women who developed dementia com-
pared with those who did not. After age 70 years, the
BMI slope decreased at a similar rate irrespective of
whether dementia occurred. Furthermore, the associa-
tion between BMI trajectory and risk of dementia was
significantlyinfluencedbythepresenceoftheAPOE4
allele (B¨ackman, et al, unpublished). The rate of BMI
decline after midlife was greater in individuals with
the APOE4 allele compared with those without the
allele. However, the greatest decline was evident in
individuals with the APOE4 allele who were diag-
nosed with dementia. Although compelling, it is not](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-2-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1113
known whether these data can be extrapolated to other
populations.
Changes in BMI also appear to be associated with
clinical progression of dementia [13]. The effects of
baseline BMI and 1-year body weight change on clin-
ical progression were assessed in 2,268 individuals
with amnestic mild cognitive impairment (MCI) and
1,506 with early-stage AD. In individuals with MCI,
high BMI (≥27.5 kg/m2) was associated with higher
baseline cognitive impairment compared with moder-
ate BMI (20.0 to <27.5 kg/m2). However, high BMI
was associated with slower clinical progression than
moderate BMI. In addition, >4% weight loss in 1 year
showed a borderline association with faster clinical
progression compared with no weight change over
the same period. In AD, high BMI was associated
with higher baseline impairment, although no signifi-
cant differences were observed in clinical progression
by baseline BMI or weight change. In addition to
the aforementioned study, no decrease in BMI among
those with AD was also observed in an observational
cohort study and a clinical study [14]. These find-
ings are in accord with other studies showing that
weight loss is associated with AD risk and faster clin-
ical progression of cognitive decline [15–17]. Of note,
the association between BMI and clinical progression
varied significantly by APOE4 status in AD. In indi-
viduals without APOE4, high BMI was associated
with a slower rate of clinical progression compared
with a moderate BMI (p = 0.010). Apolipoprotein E,
the gene product of APOE, plays a central role in the
distribution and metabolism of cholesterol and triglyc-
erides, and individuals carrying the APOE4 allele
may have higher total and low-density lipoprotein
(LDL) cholesterol [18, 19]. This finding may help to
shine some light on the link between lipid metabolism,
adipose tissue, and risk for dementia.
The mechanistic basis underlying the association
between BMI and AD may be linked to the endocrine
function of adipose tissue, mediated by adipose tissue
hormones and adipokines [12]. Accumulating evi-
dence suggests that adipose tissue may play multiple
roles in the aging brain, including disease processes
leading to dementia-related pathologies [20]. Adipose
tissue produces and releases a variety of proin-
flammatory and anti-inflammatory factors, including
the adipokines leptin, adiponectin, resistin, and vis-
fatin, as well as cytokines and chemokines, such as
tumor necrosis factor-␣, interleukin-6, and monocyte
chemoattractant protein 1 [12, 21]. It is hypothesized
that inflammatory cytokines produced in midlife may
increase the risk of AD [12]. However, the picture is
complex and extensive research is required to deter-
mine the role of adipokines in relation to clinical
dementia outcomes (reviewed in [12]). Ongoing stud-
ies in this context include imaging-based measures
of brain volume, structure, and function in humans
and preclinical models of clinical dementia [12].
Adipokines, leptins, and inflammatory cytokines also
show promise as biomarkers in the development of new
nutritionally based approaches to modify the risk of
developing AD [22].
In summary, apparently conflicting evidence for the
association between adiposity, estimated using anthro-
pometric measures, and risk of AD has not yet been
fully resolved. There is a pressing need for further
research because of the global epidemic of overweight
and obesity combined with longer life expectancy of
the general population. Future research in MCI and
AD needs to embrace the importance of nutritional
factors in the design of studies. Longitudinal studies
with sufficient follow-up are required to understand
how BMI trajectory, and the role of the APOE4
and other AD alleles, influence AD risk and pro-
gression in diverse populations. In addition, studies
should include standardized measurements of adipos-
ity beyond anthropometry, and should account for
multiple confounding factors in statistical analyses.
Finally, studies are required to test biological hypothe-
ses proposed to explain the complex epidemiological
phenomena and to differentiate between ‘cause and
effect’ in relation to nutritional status in AD.
IS ALZHEIMER’S A NUTRITIONAL
DISEASE?
Raj C. Shah
The World Health Organization (WHO) broadly
defines a nutritional disease as one ‘caused by an
insufficient intake of food or of certain nutrients, by
an inability of the body to absorb and use nutrients,
or by overconsumption of certain foods’ [23]. While
this broad definition works well for obesity caused by
excess energy intake, anemia caused by insufficient
intake of iron, and impaired sight because of inad-
equate intake of vitamin A, the situation for AD is
far more complex. While a large body of evidence
demonstrates links between nutrition and AD [2],
understanding the true nature of relationships between
AD and multiple nutrients is challenging because of a
multitude of confounding and inter-dependent factors.
First, AD has a long asymptomatic phase that con-
founds understanding the nature of physiologic and](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-3-2048.jpg)
![1114 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
Fig. 1. Schematic illustration of the relationship between disease and nutritional factors. The top panel shows that a disease process may lead
to a nutrient deficiency, a relative insufficiency, for example caused by resistance to the effect of the nutrient, or an overabundance of a nutrient.
Conversely, nutrient levels may influence the disease process. The lower panels illustrate how the relationship between AD and nutritional status
is confounded by many variables, including complex feedback loops, the involvement of multiple inter-related nutrients, and the presence of
comorbid diseases.
nutritional changes that occur before symptoms appear
and AD is clinically diagnosed [24, 25]. Indeed, mod-
eling of biomarker changes over the course of AD
suggests that important pathophysiological changes
during the preclinical phase may account for about
half of the total duration of disease in an individ-
ual [25]. This is an important observation because
measurements of cognitive decline are most imprecise
during the preclinical phase [25]. Second, the relation-
ship between disease and nutrient status is complex
and multi-dimensional, in that AD can influence nutri-
ent status and nutrient status may contribute to AD
pathophysiology. In other words, it is challenging to
discriminate between ‘cause’, i.e., the effect of a spe-
cific nutrient on AD, and ‘effect’, i.e., the effect of
AD on the levels of a specific nutrient. It is, therefore,
difficult to delineate the relationship between disease
and nutritional factors (Fig. 1). The challenge of deter-
mining causality is confounded because patients with
AD often have multiple comorbidities that may influ-
ence or be influenced by nutritional status, and multiple
nutrients may be involved in complex inter-related pro-
cesses (Fig. 1).
Changes in the levels of one particular nutrient can-
not be viewed in isolation because levels of other
nutrients may be altered by compensatory mecha-
nisms. Such complexity means that modeling in AD
needs to discriminate between ‘cause and effect’ and
to quantify nutritional status in terms of ‘deficiency or
insufficiency’. Moreover, deficiency or insufficiency
cannot be seen simply in terms of dietary input because
nutritional status may be influenced by the pathologic
processes, such as synapse loss, that characterize AD
[26, 27].
Standard modeling techniques for determining
causality may be inadequate to describe the role of
nutritional status in the onset and progression of AD.
Classically, the relationship between a disease and
causal factors may be assessed using Bradford Hill cri-
teria [28]. The strength of causal relationships between
AD and nutrient status should be tested using the
criteria of consistency, specificity, temporality, bio-
logic gradient, plausibility, coherence, experiment,
and analogy. However, in the setting of AD, most
studies conducted to date have not systematically col-
lected nutritional data to generate a sufficiently robust
dataset to allow causal relationships to be definitively
described.
Determination of a specific nutritional need,
amenable to intervention with a medical food, may
provide new management options for patients with
AD. According to FDA guidance, a medical food is
intended for the specific dietary management of a
disease or condition for which distinctive nutritional](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-4-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1115
requirements, based on recognized scientific prin-
ciples, are established by medical evaluation [29].
Following this guidance, is it possible to characterize
AD as a disease with distinctive nutritional require-
ments? Other contributing authors in this manuscript
summarize the growing body of evidence showing that
nutritional factors are important in the risk of develop-
ing AD and the rate of clinical progression. However,
the challenge of characterizing the specific nutritional
requirement remains.
A new approach is required to improve the mod-
els used to determine causality. New models need to
take into account the complex scenarios influencing
the relationship between nutritional status and AD in
the clinical setting. In this regard, it is important that
candidate effects of AD on nutrient requirements are
driven by data from human studies and are clearly
characterized by disease stage. In addition, Mendelian
randomization should be used to integrate genetic
information into traditional epidemiologic methods in
studies looking at the importance of nutritional fac-
tors over time. Such an approach recently has been
used to investigate genetic predisposition to increased
levels of blood lipids and the risk of late-onset AD
[30]. The design of nutritional-based research in AD
could be enriched by conducting neuropathology-wide
association studies looking at brain/plasma levels of
specific nutrients of interest [31]. Finally, systems biol-
ogy and/or efficient modeling approaches are needed
to characterize disease-related perturbations in nutrient
homeostasis.
In conclusion, a systematic plan will help to iden-
tify and address gaps in the evidence needed to state
that AD is associated with nutrient changes. Until such
research efforts are undertaken, significant resources
may be invested in studies with minimal chance for sig-
nificant impact. With current approaches, a significant
finding may be likely due to luck or chance. There-
fore, in the near term, replication studies are required
to confirm such findings before any changes to clinical
practice or health policy guidelines are implemented.
The evidence base guiding health management deci-
sions must be robust.
MEDITERRANEAN-TYPE DIET: DIETARY
PATTERNS AND COGNITIVE FUNCTION
Nikolaos Scarmeas
Unravelling the complexity of nutritional fac-
tors in AD may be facilitated by the systematic
study of dietary patterns. Such an approach could
capturethemultidimensionalityofnutrient-relatedfac-
tors by reducing confounding factors and integrating
complex or subtle interactions between dietary compo-
nents [32]. In addition, studies of dietary patterns may
reduce methodological flaws, such as multiple testing
and co-linearity, and are useful when well-developed
hypotheses for particular dietary elements do not exist.
Studies of the influence of the Mediterranean-type
diet (MeDi) on the risk of AD, MCI, and AD mor-
tality have contributed to our understanding of the
importance of nutritional factors [33–36]. The MeDi
is characterized by high intake of vegetables, legumes,
fruits, and cereals, a high intake of unsaturated fatty
acids, but low intake of saturated fatty acids, a moder-
ately high intake of fish, a low-to-moderate intake of
dairy products, a low intake of meat and poultry, and
a regular but moderate consumption of alcohol. These
studies showed that dietary patterns have a significant
association with risk for AD. Among community-
based individuals without dementia, higher adherence
to a MeDi was associated with a lower risk for AD
(hazard ratio [HR], 0.91; 95% confidence interval
[CI], 0.83–0.98; p = 0.015) [33]. Data also showed that
higher adherence to a MeDi is associated with reduced
risk for developing MCI and with reduced risk for MCI
conversion to AD [34]. Furthermore, it was shown that
higher adherence to a MeDi is associated with lower
mortality in AD [35]. The mean duration of survival
was 6.6 years for patients with AD with the lowest
adherence, 7.9 years for those with middle adherence,
and 10.5 years for those with the highest adherence to
a MeDi.
It is important to consider nutritional status as a
whole in the context of AD [37–40]. When a study
demonstrates an association between a dietary pattern
and a particular health outcome, although important
for public health, it is hard to know which particular
nutrient or food or food group, or any other aspect
of nutrition, is responsible for the noted relation. For
example, statistical analysis showed that in adjusted
models, none of the individual components of a MeDi
was a significant AD predictor, suggesting that the
effect of the whole may be more than its individual
constituents [33].
The validity of the MeDi–cognition relation is
another related issue. Confidence in scientific find-
ings is higher when associations are shown to be
reliable in multiple studies, settings, and populations.
The replicability of the initial findings relating a
MeDi with cognitive performance was addressed in
a meta-analysis of relevant studies that addressed sim-
ilar questions [41]. High adherence to a MeDi was](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-5-2048.jpg)
![1116 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
consistently associated with reduced risk for stroke
(relative risk [RR] 0.71, 95% CI 0.57–0.89), depres-
sion (RR 0.68, 95% CI 0.54–0.86), and cognitive
impairment (RR 0.60, 95% CI 0.43–0.83). Moderate
adherence was similarly associated with reduced risk
for depression and cognitive impairment, whereas the
protective trend for stroke was only marginal [41].
Additionally, a dose-response effect for a MeDi on
outcomes was evident. Based on these findings, the
authors concluded that high adherence to a MeDi,
seems to have beneficial effects on several central ner-
vous system (CNS)-related functions.
Regarding future research, in view of the inherent
limitations of cross-sectional epidemiological stud-
ies, prospective, longitudinal, cohort designs with
adequate follow-up and meticulous data collection
(potentially considered together after appropriate har-
monization and/or in the form of a meta-analytic
approach) would strengthen the current state of knowl-
edge. It is also important to consider other potentially
confounding factors that may influence the effect of
diet on AD. For example, in a study of community-
dwelling elders without dementia, both higher MeDi
adherence and higher physical activity were inde-
pendently associated with reduced risk for AD [42].
Individuals adhering to the diet and participating in
physical activity had a lower risk of AD than those
neither adhering to the diet nor participating in phys-
ical activity (HR 0.65 [95% CI 0.44–0.96]; p = 0.03
for trend). Other such potential confounders should be
considered in future studies.
Despite the apparent advantages of studying dietary
patterns, the limitations of observational studies
remain. Therefore, randomized controlled intervention
studies are clearly needed to investigate experimental
manipulation of dietary exposure. The design of future
studies should also consider using a range of methods
to determine how nutrient and dietary status modifies
different pathologic processes and biological pathways
within the CNS [43]. For example, magnetic resonance
imaging (MRI) was employed successfully to show
that higher adherence to MeDi was associated with
reduced cerebrovascular disease burden, specifically
MRI infarcts [44] and white matter hyperintensities
[43]. Such studies may be useful for strengthening our
biological understanding of the relation between diet
and pathologic processes in the CNS.
Inconclusion,integratinglongitudinalepidemiolog-
ical data with biomarkers of disease, including brain
imaging technology, together with randomized con-
trolled interventions may provide greater insights into
progressiveandsubtleneurologicalchangesassociated
with dietary factors in individuals at risk for AD. This
approach will help to determine the effect of MeDi
and other dietary patterns on the occurrence and course
of AD.
ROLE OF OXIDATIVE STRESS AND
ANTIOXIDANTS IN AD
Xiongwei Zhu
Agreaterunderstandingofthemechanismsinvolved
in nutritional influences on AD risk and progression
will help to better inform possible interventional strate-
gies. This point is clearly illustrated by studies of
oxidative stress and antioxidants in AD, which have
helped to refine how vitamin E is viewed as a potential
therapeutic in this setting [45].
Oxidative stress occurs when the intracellular capac-
ity for removing free radicals is exceeded, leading
to modification of DNA, lipids, polysaccharides, and
proteins, and to changes in redox homeostatic bal-
ance. Oxidative stress is a prominent and early feature
in AD pathology [46]. A study involving individu-
als with Down syndrome showed that oxidative stress
occurs earlier than neurofibrillary abnormalities and
precedes amyloid pathology by decades [47]. The
authors concluded that increased levels of oxidative
damage occur prior to the onset of both tau- and
amyloid- deposition. The same authors also showed
that increased oxidative damage is an early event in
AD that in fact decreases after lesion formation. In
addition, other studies have shown that oxidative stress
mediates amyloid- production: both amyloid- pro-
tein precursor and amyloid- increased by 3-4-fold
after an oxidative insult [48, 49]. Oxidative stress also
causes increased tau phosphorylation, facilitates the
conformational conversion and assembly of tau fibrils,
and impairs the proteasomal and lysosomal activity
that may lead to progressive accumulation of protein
deposits. Indeed it has been proposed that oxidative
stress, rather than amyloid- or tau, precipitates the
pathogenesis of AD, especially the most abundant spo-
radic forms [50, 51].
Interestingly, many of the pathogenic factors such
as oxidative damage, mitochondrial dysfunction, and
accumulationofamyloid-arefoundatsynaptictermi-
nals in AD brain and models, and are associated with
synaptic dysfunction [49]. This is important because
synaptic damage is a critical factor in cognitive decline
during aging and progression of AD [49]. Studies
have shown levels of presynaptic and postsynaptic pro-
teins are decreased in patients with AD compared with](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-6-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1117
Fig. 2. Schematic showing prevention or amelioration of oxidative
stress as potential therapeutic targets in AD.
age-matched controls and that brain regions known to
be affected in AD suffer the greatest loss of synapses
and synaptic proteins [49].
There is good evidence linking oxidative stress with
synaptic dysfunction and loss [49, 52, 53]. For exam-
ple, a mouse model of AD showed loss of postsynaptic
proteins was associated with increased oxidation [53].
This effect may involve loss of the omega-3 fatty acid
docosahexaenoic acid (DHA), which is highly vulner-
able to oxidative damage [53]. Extrapolation of these
findings suggests that dietary deficiency of DHA may
be a relevant and modifiable risk factor in AD [53].
Studies using human postmortem frontal cortex from
individuals with MCI or AD have also shown a correla-
tion between markers of oxidative stress and a decline
in Mini-Mental Status Examination scores, suggesting
a role for oxidative stress in AD-related synaptic loss
[52]. Of note, oxidative stress was more localized to the
synapses. Levels of endogenous antioxidants appear to
decline to levels that are insufficient to neutralize rising
antioxidant levels. These findings suggest increasing
brain levels of antioxidants may be helpful in slow-
ing or preventing synaptic damage caused by oxidative
stress (Fig. 2).
Evidence supporting a key role for oxidative stress
in AD pathology has provided a compelling rationale
to investigate the therapeutic potential of antioxi-
dants, including Gingko biloba, vitamin E, estrogen,
lipoic acid, non-steroidal anti-inflammatory drugs,
tenilsetam, acetyl-L-carnitine, and selegilene, for the
protection of neuronal membranes and maintenance of
metabolic control. Antioxidant therapy is purported to
reduce amyloid- and tau protein and their deposits,
and synaptic changes by limiting oxidative stress-
related damage, but at present evidence for clinical
benefit is limited [54, 55]. Among these antioxidants,
vitamin E is perhaps the most extensively studied.
Vitamin E is a term to describe eight, fat-soluble
derivatives of tocopherol and tocotrienol. Of these,
alpha-tocopherol is most commonly used in supple-
ment form and the only form used in trials of patients
with AD or MCI. However, a systematic review found
noconvincingevidencethatalpha-tocopherolisofben-
efit in the treatment of AD or MCI [56], although
none of the completed trials targeted individuals with
marginal vitamin E status, who may be the population
most likely to benefit from vitamin E supplementa-
tion. It should be emphasized that the oxidative stress
hypothesis in the pathogenesis of AD is far from
being extensively tested and further studies are still
urgently needed to determine how and where antiox-
idants should be used in the prevention and treatment
of AD. Furthermore, genome-wide association stud-
ies point to the need to consider multiple aspects of
AD pathology in the design of future research [57]. Of
note, genetic variation in the clusterin (apolipoprotein
J) gene appears to be associated with the pathogene-
sis of AD via various pathways, including amyloid-
aggregation and clearance, lipid metabolism, and neu-
roinflammation [58]. Such findings may provide new
opportunities for therapeutic and nutritional interven-
tions in AD.
In conclusion, oxidative stress contributes to loss of
neuronalintegrityinAD.Dietarynutrientswithantiox-
idant properties may have positive effects in AD and
thoseatriskforADbyreducingoxidativestress,partic-
ularly when used in combination. The preventive and
therapeutic potential of antioxidants in AD remains to
be fully defined.
NUTRITIONAL NEEDS FOR
MAINTAINING MEMBRANE INTEGRITY,
INCLUDING NEW DIETARY APPROACHES
Martha Clare Morris
In the CNS, phospholipid bilayers integrate with
lipids (e.g., choline) and proteins to form neuronal
membranes [59]. Neuronal functioning is profoundly
affected by degeneration and changes affecting the
dynamic neuronal membrane structure [59–61]. Pre-
clinical experiments have provided evidence to show
that lowering the availability of key nutrients can have
an adverse effect on neuronal structure and function;
for example, synaptic proteins involved in learning
and memory are down-regulated in the DHA-deficient
mouse brain [62] and neurite growth and synapto-
genesis in cultured hippocampal neurons are inhibited](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-7-2048.jpg)
![1118 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
Table 1
Evidence for the role of specific nutrients required to maintain a healthy brain
Nutrient Food sources
Strong evidence Dietary tocopherols – low deleterious Nuts, oils, seeds, green leafy vegetables,
whole grains
DHA – low deleterious Fish
Folate – low deleterious Vegetables, whole grains
Saturated fat – high deleterious
Unsaturated fat – high beneficial
Commercial products, baked goods, red
meats, high fat dairy
Moderate/limited evidence Carotenoids (-carotene, lutein,
lycopene)
Green leafy vegetables, bright-colored fruit,
vegetables
Flavonoids Berries
Vitamin D Fish, dairy
Trans fat Commercial products, baked goods
Monosaturated fat Olive oil
Polyphenols Olive oil, red wine, teas, vegetables, fruit
by prenatal depletion of DHA [63]. Moreover, many
studies in humans have shown that brain structure and
function are influenced by nutrients obtained from the
diet [64, 65]. It follows therefore, that the CNS requires
specific nutrients to maintain neuronal integrity and
to support everyday brain functions, including cogni-
tion [61].
Table 1 summarizes the strength of evidence for
the role of specific nutrients in brain functions. The
level of evidence is strong for dietary tocopherols,
where a low intake has been shown to be deleteri-
ous for brain health, DHA (low intake is deleterious),
folate (low intake is deleterious), and fatty acids (a
high intake of saturated fatty acids is deleterious,
whereas, a high intake of unsaturated fatty acids is
beneficial) [66]. A healthy diet is therefore one of
the key principles recommended for AD prevention
[5]. In addition, epidemiological data have shown
an association between adherence to certain healthy
dietary patterns, for example the MeDi or Dietary
Approaches to Stop Hypertension (DASH) diets, and
slower cognitive decline and lower risk of develop-
ing dementia, including AD [33, 67–69]. However,
although a growing number of epidemiological studies
indicate nutrition is related to the development of AD
[70], dietary recommended daily amounts (RDAs) are
not optimized to meet the specific nutritional require-
ments of the brain [71, 72]. The optimal nutrient level
for brain functioning and prevention of neurodegener-
ation may be very different from the level required to
avoid deficiency.
SeveralnutrientsareofspecialinterestinAD,partic-
ularly those required for the maintenance of neuronal
integrity, including antioxidants and fatty acids. As
discussed by Xiongwei Zhu in this article, antiox-
idants, specifically tocopherols, may reduce plaque
formation, neurofibrillary tangles, and synapse loss.
Although there are extensive preclinical data providing
a scientific basis for antioxidant strategies to prevent
AD, epidemiological studies have generated conflict-
ing results. For example, studies have shown that food
sources of tocopherols are protective, whereas vitamin
E supplements (␣-tocopherol) are not [31, 56]. Dif-
ferences in the biological effects between tocopherols
(␣, , ␥, and δ) may explain this discrepancy [31,
73]. Understanding the differences between different
forms of vitamin E may inform future studies in AD
prevention [73–75]. The most common supplemental
form of vitamin E is ␣-tocopherol, which is a potent
antioxidant within cell membranes [73]; however, ␥-
tocopherol, the major form of tocopherol provided by
North American diets, has been shown to have anti-
amyloidogenic, anti-inflammatory, and anti-nitrative
capacities [31, 76]. At least in the preclinical setting,
␣- and ␥-tocopherols work synergistically [77, 78],
so it is important that future randomized trials should
consider the contribution of ␥-tocopherol [31]. Fur-
thermore, for dietary management, vitamin E should
be obtained from foods, rather than taken as separate
supplements [5].
Changes in the composition and levels of fatty acids
also have important implications on neuronal integrity
during aging and the development of AD [79–81].
Polyunsaturated fatty acids (PUFAs), such as DHA, are
essential to support neuronal integrity and brain func-
tion [79]; however, studies have shown that increasing
age is associated with a progressive decline in PUFA
composition, including DHA and arachidonic acid
[80]. Preclinical studies have shown that dietary DHA
increases brain levels of DHA, leading to beneficial
changes in cerebral functions relevant to the patho-
physiology of AD [82–89], including hippocampal
nerve growth, improved fluidity of synaptic mem-
branes, induction of antioxidant enzymes, increased](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-8-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1119
transcription of transthyretin (an amyloid protein scav-
enger), and greater cerebral blood volume. In addition,
these studies showed that increasing levels of DHA in
the brain leads to decreased oxidation of lipid mem-
branes, less ischemic damage to neurons, decreased
inflammation, lower amyloid burden, reduced synaptic
loss, and mitigation of impaired learning.
The central role of lipids in maintaining neuronal
integrity has clear implications for dietary manage-
ment for AD prevention and management. A high
ratio of saturated/unsaturated fatty acids in the diet
leads to an increase in LDL and a decrease in
high-density lipoprotein cholesterol; this change may
significantly alter the risk of developing AD [70,
79]. Preclinical studies have shown that diets high
in saturated fat/cholesterol level are associated with
impaired memory, amyloid- deposition and plaque
formation, neuroinflammation, neurotoxicity, and an
increase in brain lesions [90–96]. Furthermore, choles-
terol appears to play a central role in AD, and of
particular interest, the most important genetic risk
factor for AD is the APOE4 allele, which is prin-
cipally responsible for regulating cholesterol transport
in the brain [70]. Healthy diet regimes, such as DASH
(developed to reduce blood pressure) and the MeDi (a
culturally-based diet), recommend low intake of satu-
rated fats and a high intake of PUFAs [97].
In summary, accumulating evidence suggests that
diet and nutrition status influence neuronal membrane
integrity and risk for AD. Maintaining a healthy diet,
designed to support neuronal membrane integrity, may
reduce the risk of developing AD [5].
NUTRIENT LEVELS IN AD
John Sijben
Two major factors are thought to contribute to a
specific nutritional need in patients with early AD:
increased loss of synapses and a lower nutritional
status. Synapse loss is an early feature in the pro-
gression of AD [26, 98–105] and is associated with
significant functional deficits [106, 107]. Furthermore,
loss of neuronal structure is associated with phospho-
lipid changes in the brain and functional deterioration
[108]. The neuronal membrane is the principal site of
action for many neuronal activities. The biochemical
and biophysical properties of the neuronal membrane
are important determinants of proper neuronal func-
tion, but can be subject to alterations induced by
nutritional compounds [61].
The formation of new neuronal membranes and the
maintenance of membrane composition and structure
are highly dynamic processes that occur continuously
throughout life [109]. These processes rely upon a sus-
tained supply of neuronal membrane precursors and
cofactors, largely provided by the diet. It has been
known for many years that neuronal membrane syn-
thesis is controlled by the availability of rate-limiting
dietary precursors [27, 61, 110]. Preclinical exper-
iments have shown that a combination of specific
dietary precursors and cofactors increase the forma-
tion of neuronal membrane structures [86, 111, 112].
Conversely, lowering the availability of key nutrients
can have an adverse effect on neuronal structure and
function [53, 62, 63, 113].
Patients with AD have lower levels of specific
nutrients required to support the formation of phos-
pholipids and maintain neuronal membrane integrity
[114], which is highlighted by systematic reviews and a
meta-analysis comparing plasma levels of micronutri-
ents and fatty acids in patients with AD and cognitively
intact elderly controls [114–116]. The analyses clearly
demonstrated that levels of circulating folate and vita-
mins (A, B12, C, D, and E), PUFAs (DHA and
eicosapentaenoic acid) and selenium, are significantly
lower in patients with AD than in controls (Fig. 3).
Additional analysis showed that lower nutrient status
in AD is independent of nourishment status [114].
Other studies found lower plasma uridine levels in
patients with AD compared with controls [117–120].
This is a particularly relevant finding in this context
because circulating uridine is the source of brain cyti-
dine triphosphate, which plays an important role in
phospholipid synthesis [27]. While infants obtain uri-
dine from breast or formula milk, adults rely on hepatic
synthesis because dietary uridine provided by RNA
is not readily bioavailable. Circulating uridine crosses
the blood-brain barrier and after entering brain cells it
is phosphorylated, initially to uridine monophosphate,
and retained. Extensive research has shown that uridine
administered with other nutrients (DHA and choline)
enhances the formation and function of synaptic struc-
tures, providing a scientific rationale for nutritional
support for patients with AD (reviewed in [27] and
[121]).
The lower plasma nutrient levels indicate that
patients with AD have impaired systemic availabil-
ity of several nutrients. Consequently, lower systemic
availability of nutrients may reduce levels in the brain.
This appears to be supported by evidence from studies
that have shown reduced availability of nutrients in the
cerebrospinal fluid (CSF) of patients with AD [122].](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-9-2048.jpg)
![1120 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
Fig. 3. Data from a systematic review and meta-analysis comparing plasma levels of micronutrients and fatty acids in AD patients with those
in cognitively intact elderly controls [114–120].
Specifically, the systematic review and meta-analysis
showed lower brain levels of DHA and choline, and
lower CSF levels of folate and vitamin C [123].
Another study reported lower levels of uridine in the
CSF [122]. It has also been shown that lipid-bound
choline homeostasis is shifted toward catabolism in
AD, suggesting a compensatory mechanism triggered
by lower availability of choline [124–127]. This issue
is further compounded because brain uptake of choline
decreases with aging [128]. Overall, lower availability
of these specific nutrients reduces the capacity to form
neuronal membranes and synapses (Fig. 4).
There are several reasons for lower nutrient status
in patients with AD compared with controls. Dietary
intake of nutrients may be affected by worsening of
appetite, taste, and smell, which lead to reduced food
consumption, food neglect, changes in food prefer-
ences, and poor food choice [129–131]. Low nutrient
levels in patients with AD are not only attributable to
changes in dietary intake, and it is now recognized that
metabolic changes also contribute to a worsening nutri-
entstatus.ThismeansthatasADprogresses,apatient’s
abilitytometabolizeorsynthesizekeynutrientsmaybe
diminished, for example, by having a reduced ability to
convert ␣-linolenic acid to DHA [132]. Furthermore,
lower dietary intake of B vitamins (folate, vitamin B12,
and vitamin B6) may lead to high levels of homo-
cysteine in patients with AD [133], which in turn,
reduces the methylation capacity of many methyltrans-
ferases, resulting in lower availability of DHA and
choline synthesized via the phosphatidylethanolamine
N-methyltransferase pathway [61]. Another potential
reason for low nutrient levels in patients with AD is
impaired absorption and uptake of key nutrients [3].
For example, aging is associated with less efficient
absorption of vitamin B12 because of reduced acidity
in the stomach [134–136], and, in AD, tissue availabil-
ity is further reduced because a lower percentage of
B12 is present in the active holotranscobalamin form
[137, 138]. This means that even if dietary intake is
adequate, the availability of nutrients where they are
required, i.e., the brain, may be insufficient at a time
when nutrient requirement is increased because of neu-
ronal membrane degradation [3].
Accumulating evidence suggests there is a specific
nutritional need in AD [3]. Souvenaid®, a dietary
food for special medical purposes, was developed to
address this need based on years of research [61].
Preclinical studies have shown that increasing the sup-
ply of a specific combination of nutrients supports
the formation and function of neuronal membranes
and improves measures of cognitive performance [61].
Souvenaid provides nutritional precursors and cofac-
tors (DHA 1200 mg, eicosapentaenoic acid 300 mg,
uridine monophosphate 625 mg, choline 400 mg, folic
acid 400 mcg, vitamin B6 1 mg, vitamin B12 3
mcg, vitamin C 80 mg, vitamin E 40 mg, selenium
60 mcg, and phospholipids 106 mg), at levels that
cannot be achieved by diet alone [61]. Clinical stud-
ies have shown that Souvenaid preserves functional](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-10-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1121
Fig. 4. Schematic model to show lower availability of nutrients required for membrane and synapse formation in AD.
connectivity and improves memory performance in
patients with early AD [139–141]. Furthermore, Sou-
venaid significantly increases blood levels of nutrients
and phospholipids [140–141; (Rijpma et al, unpub-
lished)]. Interestingly, plasma phospholipids have been
shown to be biomarkers for diagnosis of preclini-
cal AD [142] and most of the phosphatidylcholine
species reported by Mapstone and colleagues in
this context are significantly increased by Souvenaid
[143]. Souvenaid is now being studied in the set-
ting of prodromal AD [144] in the LipiDiDiet
trial [145]. The primary endpoint of the study is
cognitive performance during 24 months of inter-
vention and progression to dementia is a secondary
endpoint.
In summary, data suggest that patients with AD
have distinctive nutritional requirements that may be
addressed by specific dietary management. It is also
apparent that the nutrient requirement cannot easily
be met with diet alone and, therefore, there is a clear
rationale for a specific combination of nutrients that
may be offered as a medical food.
CONCLUSIONS AND VIEWPOINT
Converging lines of scientific, clinical, and epi-
demiological evidence indicate an association between
dietary/nutritional factors and AD. In this proceedings
article, we have discussed several topics that demon-
strate the importance of nutrition in AD and highlight](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-11-2048.jpg)
![1122 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
the need for additional systematic research in this area.
In addition, we have emphasized the complexity of
the task in hand, which is confounded by a multi-
plicity of dynamic and inter-related factors interacting
over a long period of time. At a macroscopic level,
long-term, longitudinal data have demonstrated a rela-
tionship between BMI trajectory and AD risk [10].
Along the same line of evidence, there is an emerging
link between adiposity, metabolic syndromes, and risk
ofdementia[12,20].Theevidencebaseisstrengthened
by epidemiological data showing the impact of partic-
ular dietary patterns and risk of AD. The archetypical
example is adherence to the MeDi, which is associated
withlowerriskforMCIandAD[33].Detailedanalyses
of these data lead to the conclusion that the potentially
beneficial effect of the MeDi could be attributable to a
combination of nutrients, rather than a single one. It is
interesting to note that the levels of nutrients in the cir-
culation and brain are lower in patients with AD than
in age-matched controls [114]. Specifically, new data
have shown that patients with AD have lower levels of
the specific nutrients required to support the formation
of phospholipids and to maintain neuronal integrity.
Furthermore, preclinical models of AD have shown
there is an increased requirement for specific nutrients
to counter synapse loss, however, nutrient availability
in the circulation and brain may be inadequate to meet
this need [3, 61].
Research into possible links between nutritional fac-
tors and risk of AD has been accompanied by the
development of interventional strategies ranging from
single-agent supplements to dietary regimes specif-
ically developed for individuals at risk from AD.
Studies of single-agent nutritional supplements have
produced largely equivocal results and the consensus
is that overall nutritional status should be improved
by providing a combination of specific nutrients [5].
Providing single high-dose nutrient supplements, e.g.,
vitamin E in nutritionally replete individuals, appears
not to be effective and rationally designed combina-
tions of nutrients or use in individuals with marginal
nutritional status may achieve better outcomes. Based
on the available evidence, there appears to be a clini-
cal need to ensure that nutritional intake is optimized
to reduce the risks of AD onset and progression
[5]. Both dietary quality (e.g., a MeDi providing the
right combination of nutrients) and bodyweight tra-
jectory are important considerations in the context of
AD risk and progression. Although RDAs for nutri-
ents are not appropriate as guidance for the specific
needs of the brain, dietary intake is an important
variable.
Overall, it can be concluded that there is a need for
more information on the causes of nutritional changes
in individuals at risk of progression to AD before
clinical symptoms become apparent. It is important,
therefore, that nutritional markers and dietary intake
should be measured in future studies. There is con-
sensus among the authors that nutritional deficits are
associated with AD, but more work is needed to deter-
mine cause and effect. Appropriately designed diets or
nutritional interventions, such as Souvenaid, may have
a role to play to address the specific nutritional need
before or after the clinical onset of AD, but more work
is needed on various aspects of their clinical–cognitive
effectiveness. As a result of this roundtable discussion,
a new PIA on nutrition in dementia was formed within
the ISTAART. The objectives of this initiative include:
to develop and advance clinical and research applica-
tions of nutrition in AD and related disorders; to create
and promote dedicated research sessions on the topic
at scientific conferences; to foster development of con-
sensus criteria for nutrition research and interpretation
of relevant findings; and to facilitate the creation of
multi-study collaborations.
ACKNOWLEDGMENTS
The authors received the following support: Deb-
orah R. Gustafson: Swedish Research Council
for Health, Working Life and Welfare (AGECAP
2013-2300) and EU 7th framework LipiDiDiet
project (FP7/2007-2015) under grant agreement no.
211696; Nikolaos Scarmeas: 189 10276/8/9/2011
from the ESPA-EU program Excellence Grant
(ARISTEIA) which is co-funded by the European
Social Fund and Greek National resources; and
Y2/oικ.51657/14.4.2009 from the Ministry for
Health and Social Solidarity (Greece); Raj C Shah:
The Illinois Department of Public Health; Morris MC:
National Institute on Aging and National Institute on
Environmental Health Sciences.
Authors’ disclosures available online (http://j-
alz.com/manuscript-disclosures/15-0084r1).
REFERENCES
[1] Ballard C, Gauthier S, Corbett A, Brayne C, Aarsland D,
JonesE(2011)Alzheimer’sdisease.Lancet377,1019-1031.
[2] CardosoBR,CominettiC,CozzolinoSM(2013)Importance
and management of micronutrient deficiencies in patients
with Alzheimer’s disease. Clin Interv Aging 8, 531-542.
[3] Mi W, van Wijk N, Cansev M, Sijben JW, Kamphuis PJ
(2013) Nutritional approaches in the risk reduction and man-
agement of Alzheimer’s disease. Nutrition 29, 1080-1089.](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-12-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1123
[4] Kamphuis PJ, Scheltens P (2010) Can nutrients prevent or
delay onset of Alzheimer’s disease? J Alzheimers Dis 20,
765-775.
[5] Barnard ND, Bush AI, Ceccarelli A, Cooper J, de Jager
CA, Erickson KI, Fraser G, Kesler S, Levin SM, Lucey B,
Morris MC, Squitti R (2014) Dietary and lifestyle guidelines
for the prevention of Alzheimer’s disease. Neurobiol Aging
35(Suppl 2), S74-S78.
[6] Cooper JK (2014) Nutrition and the brain: What advice
should we give? Neurobiol Aging 35 (Suppl 2), S79-S83.
[7] Whitmer RA, Gunderson EP, Barrett-Connor E, Quesen-
berry CP Jr, Yaffe K (2005) Obesity in middle age and future
risk of dementia: A 27 year longitudinal population based
study. BMJ 330, 1360.
[8] Gustafson DR, B¨ackman K, Joas E, Waern M, ¨Ostling S,
Guo X, Skoog I (2012) 37 years of body mass index and
dementia: Observations from the prospective population
study of women in Gothenburg, Sweden. J Alzheimers Dis
28, 163-171.
[9] Gustafson DR, Luchsinger JA (2013) High adiposity: Risk
factor for dementia and Alzheimer’s disease? Alzheimers
Res Ther 5, 57.
[10] Emmerzaal TL, Kiliaan AJ, Gustafson DR (2015) 2003-
2013: A decade of body mass index, Alzheimer’s disease,
and dementia. J Alzheimers Dis 43, 739-755.
[11] Qizilbash N, Gregson J, Johnson ME, Pearce N, Douglas
I, Wing K, Evans SJ, Pocock SJ (2015) BMI and risk of
dementia in two million people over two decades: A ret-
rospective cohort study. Lancet Diabetes Endocrinol, doi:
10.1016/S2213-8587(15)00033-9.
[12] Kiliaan AJ, Arnoldussen IA, Gustafson DR (2014)
Adipokines: A link between obesity and dementia? Lancet
Neurol 13, 913-923.
[13] Besser LM, Gill DP, Monsell SE, Brenowitz W, Meranus
DH, Kukull W, Gustafson DR (2014) Body mass index,
weight change, and clinical progression in mild cognitive
impairment and Alzheimer disease. Alzheimer Dis Assoc
Disord 28, 36-43.
[14] Gu Y, Scarmeas N, Cosentino S, Brandt J, Albert M, Blacker
D, Dubois B, Stern Y (2014) Change in body mass index
before and after Alzheimer’s disease onset. Curr Alzheimer
Res 11, 349-356.
[15] Buchman AS, Wilson RS, Bienias JL, Shah RC, Evans DA,
Bennett DA (2005) Change in body mass index and risk of
incident Alzheimer disease. Neurology 65, 892-897.
[16] Soto ME, Secher M, Gillette-Guyonnet S, Abellan van Kan
G, Andrieu S, Nourhashemi F, Rolland Y, Vellas B (2012)
Weight loss and rapid cognitive decline in community-
dwelling patients with Alzheimer’s disease. J Alzheimers
Dis 28, 647-654.
[17] Cronk BB, Johnson DK, Burns JM, Alzheimer’s Disease
Neuroimaging, Initiative (2010) Body mass index and cog-
nitive decline in mild cognitive impairment. Alzheimer Dis
Assoc Disord 24, 126-130.
[18] Mahley RW, Weisgraber KH, Huang Y (2006) Apolipopro-
tein E4: A causative factor and therapeutic target in
neuropathology, including Alzheimer’s disease. Proc Natl
Acad Sci U S A 103, 5644-5651.
[19] Sing CF, Davignon J (1985) Role of the apolipoprotein
E polymorphism in determining normal plasma lipid and
lipoprotein variation. Am J Hum Genet 37, 268-285.
[20] Gustafson DR (2010) Adiposity hormones and dementia. J
Neurol Sci 299, 30-34.
[21] Fantuzzi G (2005) Adipose tissue, adipokines, and inflam-
mation. J Allergy Clin Immunol 115, 911-919.
[22] Zeki Al Hazzouri A, Stone KL, Haan MN, Yaffe K (2013)
Leptin, mild cognitive impairment, and dementia among
elderly women. J Gerontol A Biol Sci Med Sci 68, 175-180.
[23] World Health Organization. Heath topics: Nutrition dis-
orders. http://www.who.int/topics/nutrition disorders/en/.
Accessed September 2014.
[24] Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S,
FaganAM,IwatsuboT,JackCRJr,KayeJ,MontineTJ,Park
DC, Reiman EM, Rowe CC, Siemers E, Stern Y, Yaffe K,
Carrillo MC, Thies B, Morrison-Bogorad M, Wagster MV,
Phelps CH (2011) Toward defining the preclinical stages of
Alzheimer’s disease: Recommendations from the National
Institute on Aging-Alzheimer’s Association workgroups on
diagnostic guidelines for Alzheimer’s disease. Alzheimers
Dement 7, 280-292.
[25] Jack CR Jr, Knopman DS, Jagust WJ, Petersen RC,
Weiner MW, Aisen PS, Shaw LM, Vemuri P, Wiste HJ,
Weigand SD, Lesnick TG, Pankratz VS, Donohue MC, Tro-
janowski JQ (2013) Tracking pathophysiological processes
in Alzheimer’s disease: An updated hypothetical model of
dynamic biomarkers. Lancet Neurol 12, 207-216.
[26] Selkoe DJ (2002) Alzheimer’s disease is a synaptic failure.
Science 298, 789-791.
[27] Wurtman RJ, Cansev M, Sakamoto T, Ulus IH (2009) Use
of phosphatide precursors to promote synaptogenesis. Annu
Rev Nutr 29, 59-87.
[28] Bradford Hill A (1965) The environment and disease: Asso-
ciation or causation? Proc R Soc Med 58, 295-300.
[29] FDA Guidance. Draft Guidance for Industry: Frequently
Asked Questions About Medical Foods; Second Edition.
http : // www.fda.gov / Food/GuidanceRegulation/Guidance
DocumentsRegulatoryInformation / MedicalFoods/ucm054
048.htm. May 1997; May 2007; Revised August 2013;
Accessed September 2014.
[30] Proitsi P, Lupton MK, Velayudhan L, Newhouse S, Fogh
I, Tsolaki M, Daniilidou M, Pritchard M, Kloszewska I,
Soininen H, Mecocci P, Vellas B, Alzheimer’s Disease Neu-
roimaging Initiative, Williams J, GERAD1 Consortium,
Stewart R, Sham P, Lovestone S, Powell JF (2014) Genetic
predisposition to increased blood cholesterol and triglyc-
eridelipidlevelsandriskofAlzheimerdisease:AMendelian
randomization analysis. PLoS Med 11, e1001713.
[31] Morris MC, Schneider JA, Li H, Tangney CC, Nag S,
Bennett DA, Honer WG, Barnes LL (2015) Brain toco-
pherols related to Alzheimer’s disease neuropathology in
humans. Alzheimers Dement 11, 32-39.
[32] Jacques PF, Tucker KL (2001) Are dietary patterns useful
for understanding the role of diet in chronic disease? Am J
Clin Nutr 73, 1-2.
[33] Scarmeas N, Stern Y, Tang MX, Mayeux R, Luchsinger JA
(2006) Mediterranean diet and risk for Alzheimer’s disease.
Ann Neurol 59, 912-921.
[34] Scarmeas N, Stern Y, Mayeux R, Manly JJ, Schupf N,
Luchsinger JA (2009) Mediterranean diet and mild cognitive
impairment. Arch Neurol 66, 216-225.
[35] Scarmeas N, Luchsinger JA, Mayeux R, Stern Y (2007)
Mediterranean diet and Alzheimer disease mortality. Neu-
rology 69, 1084-1093.
[36] Gu Y, Nieves JW, Stern Y, Luchsinger JA, Scarmeas N
(2010) Food combination and Alzheimer disease risk: A
protective diet. Arch Neurol 67, 699-706.
[37] VandongenR,MoriTA,BurkeV,BeilinLJ,MorrisJ,Ritchie
J (1993) Effects on blood pressure of omega 3 fats in subjects
at increased risk of cardiovascular disease. Hypertension 22,
371-379.](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-13-2048.jpg)
![1124 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
[38] MoriTA,VandongenR,BeilinLJ,BurkeV,MorrisJ,Ritchie
J (1994) Effects of varying dietary fat, fish, and fish oils on
blood lipids in a randomized controlled trial in men at risk
of heart disease. Am J Clin Nutr 59, 1060-1068.
[39] Mori TA, Beilin LJ, Burke V, Morris J, Ritchie J (1997)
Interactions between dietary fat, fish, and fish oils and their
effects on platelet function in men at risk of cardiovascular
disease. Arterioscler Thromb Vasc Biol 17, 279-286.
[40] Morris MC, Evans DA, Tangney CC, Bienias JL, Schnei-
der JA, Wilson RS, Scherr PA (2006) Dietary copper and
high saturated and trans fat intakes associated with cognitive
decline. Arch Neurol 63, 1085-1088.
[41] Psaltopoulou T, Sergentanis TN, Panagiotakos DB, Ser-
gentanis IN, Kosti R, Scarmeas N (2013) Mediterranean
diet, stroke, cognitive impairment, and depression: A meta-
analysis. Ann Neurol 74, 580-591.
[42] Scarmeas N, Luchsinger JA, Schupf N, Brickman AM,
Cosentino S, Tang MX, Stern Y (2009) Physical activ-
ity, diet, and risk of Alzheimer disease. JAMA 302,
627-637.
[43] Gardener H, Scarmeas N, Gu Y, Boden-Albala B, Elkind
MS, Sacco RL, DeCarli C, Wright CB (2012) Mediterranean
diet and white matter hyperintensity volume in the Northern
Manhattan Study. Arch Neurol 69, 251-256.
[44] Scarmeas N, Luchsinger JA, Stern Y, Gu Y, He J, DeCarli
C, Brown T, Brickman AM (2011) Mediterranean diet and
magnetic resonance imaging-assessed cerebrovascular dis-
ease. Ann Neurol 69, 257-268.
[45] Vi˜na J, Lloret A, Giraldo E, Badia MC, Alonso MD (2011)
Antioxidant pathways in Alzheimer’s disease: Possibilities
of intervention. Curr Pharm Des 17, 3861-3864.
[46] Clark TA, Lee HP, Rolston RK, Zhu X, Marlatt MW, Castel-
lani RJ, Nunomura A, Casadesus G, Smith MA, Lee HG,
Perry G (2010) Oxidative stress and its implications for
future treatments and management of Alzheimer disease.
Int J Biomed Sci 6, 225-227.
[47] Nunomura A, Perry G, Pappolla MA, Friedland RP, Hirai
K, Chiba S, Smith MA (2000) Neuronal oxidative stress
precedes amyloid-beta deposition in Down syndrome. J
Neuropathol Exp Neurol 59, 1011-1017.
[48] Tamagno E, Bardini P, Obbili A, Vitali A, Borghi R, Zaccheo
D, Pronzato MA, Danni O, Smith MA, Perry G, Tabaton M
(2002) Oxidative stress increases expression and activity of
BACE in NT2 neurons. Neurobiol Dis 10, 279-288.
[49] Reddy PH, Beal MF (2008) Amyloid beta, mitochondrial
dysfunctionandsynapticdamage:Implicationsforcognitive
decline in aging and Alzheimer’s disease. Trends Mol Med
14, 45-53.
[50] Zhu X, Lee HG, Casadesus G, Avila J, Drew K, Perry G,
Smith MA (2005) Oxidative imbalance in Alzheimer’s dis-
ease. Mol Neurobiol 31, 205-217.
[51] Sutherland GT, Chami B, Youssef P, Witting PK (2013)
Oxidative stress in Alzheimer’s disease: Primary villain or
physiological by-product? Redox Rep 18, 134-141.
[52] Ansari MA, Scheff SW (2010) Oxidative stress in the
progression of Alzheimer disease in the frontal cortex. J
Neuropathol Exp Neurol 69, 155-167.
[53] Calon F, Lim GP, Yang F, Morihara T, Teter B, Ubeda O,
Rostaing P, Triller A, Salem N Jr, Ashe KH, Frautschy SA,
Cole GM (2004) Docosahexaenoic acid protects from den-
dritic pathology in an Alzheimer’s disease mouse model.
Neuron 43, 633-645.
[54] Otaegui-Arrazola A, Amiano P, Elbusto A, Urdaneta E,
Mart´inez-Lage P (2014) Diet, cognition, and Alzheimer’s
disease: Food for thought. Eur J Nutr 53, 1-23.
[55] Crichton GE, Bryan J, Murphy KJ (2013) Dietary antioxi-
dants, cognitive function and dementia–a systematic review.
Plant Foods Hum Nutr 68, 279-292.
[56] Farina N, Isaac MG, Clark AR, Rusted J, Tabet N (2012)
Vitamin E for Alzheimer’s dementia and mild cognitive
impairment. Cochrane Database Syst Rev 11, CD002854.
[57] Naughton BJ, Duncan FJ, Murrey DA, Meadows AS,
Newsom DE, Stoicea N, White P, Scharre DW, Mccarty DM,
Fu H (2015) Blood genome-wide transcriptional profiles
reflect broad molecular impairments and strong blood-
brain links in Alzheimer’s disease. J Alzheimers Dis 43,
93-108.
[58] Yu JT, Tan L (2012) The role of clusterin in Alzheimer’s dis-
ease: Pathways, pathogenesis, and therapy. Mol Neurobiol
45, 314-326.
[59] van Meer G, Voelker DR, Feigenson GW (2008) Membrane
lipids: Where they are and how they behave. Nat Rev Mol
Cell Biol 9, 112-124.
[60] Yehuda S, Rabinovitz S, Carasso RL, Mostofsky DI (2002)
The role of polyunsaturated fatty acids in restoring the aging
neuronal membrane. Neurobiol Aging 23, 843-853.
[61] van Wijk N, Broersen LM, de Wilde MC, Hageman RJ,
Groenendijk M, Sijben JW, Kamphuis PJ (2014) Targeting
synaptic dysfunction in Alzheimer’s disease by administer-
ing a specific nutrient combination. J Alzheimers Dis 38,
459-479.
[62] Sidhu VK, Huang BX, Kim HY (2011) Effects of docosa-
hexaenoic acid on mouse brain synaptic plasma membrane
proteome analyzed by mass spectrometry and (16)O/(18)O
labeling. J Proteome Res 10, 5472-5480.
[63] CaoD,KevalaK,KimJ,MoonHS,JunSB,LovingerD,Kim
HY (2009) Docosahexaenoic acid promotes hippocampal
neuronal development and synaptic function. J Neurochem
111, 510-521.
[64] Bourre JM (2006) Effects of nutrients (in food) on the struc-
ture and function of the nervous system: Update on dietary
requirements for brain. Part 1: Micronutrients. J Nutr Health
Aging 10, 377-385.
[65] Bourre JM (2006) Effects of nutrients (in food) on the
structure and function of the nervous system: Update on
dietary requirements for brain. Part 2 : Macronutrients. J
Nutr Health Aging 10, 386-399.
[66] Morris MC, Tangney CC (2010) Diet and prevention of
Alzheimer disease. JAMA 303, 2519-2520.
[67] Panza F, Solfrizzi V, Colacicco AM, D’Introno A, Capurso
C, Torres F, Del Parigi A, Capurso S, Capurso A (2004)
Mediterranean diet and cognitive decline. Public Health
Nutr 7, 959-963.
[68] Tangney CC, Li H, Wang Y, Barnes L, Schneider JA,
Bennett DA, Morris MC (2014) Relation of DASH- and
Mediterranean-like dietary patterns to cognitive decline in
older persons. Neurology 83, 1410-1416.
[69] Smith PJ, Blumenthal JA, Babyak MA, Craighead L, Welsh-
Bohmer KA, Browndyke JN, Strauman TA, Sherwood A
(2010)Effectsofthedietaryapproachestostophypertension
diet, exercise, and caloric restriction on neurocognition in
overweight adults with high blood pressure. Hypertension
55, 1331-1338.
[70] Morris MC (2009) The role of nutrition in Alzheimer’s dis-
ease: Epidemiological evidence. Eur J Neurol 16(Suppl 1),
1-7.
[71] Willett WC (1998) Nutritional Epidemiology, 2nd Edition,
Oxford University Press, New York, pp.
[72] Mertz W (1981) The essential trace elements. Science 213,
1332-1338.](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-14-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1125
[73] Morris MC, Evans DA, Tangney CC, Bienias JL, Wilson RS,
Aggarwal NT, Scherr PA (2005) Relation of the tocopherol
formstoincidentAlzheimerdiseaseandtocognitivechange.
Am J Clin Nutr 81, 508-514.
[74] Usoro OB, Mousa SA (2010) Vitamin E forms in
Alzheimer’s disease: A review of controversial and clinical
experiences. Crit Rev Food Sci Nutr 50, 414-419.
[75] Evans DA, Morris MC, Rajan KB (2014) Vitamin E,
memantine, and Alzheimer disease. JAMA 311, 29-30.
[76] Jiang Q, Christen S, Shigenaga MK, Ames BN (2001)
Gamma-tocopherol, the major form of vitamin E in the US
diet, deserves more attention. Am J Clin Nutr 74, 714-722.
[77] Liu M, Wallmon A, Olsson-Mortlock C, Wallin R, Saldeen
T (2003) Mixed tocopherols inhibit platelet aggregation in
humans: Potential mechanisms. Am J Clin Nutr 77, 700-706.
[78] Cl´ement M, Bourre JM (1997) Graded dietary levels of
RRR-gamma-tocopherol induce a marked increase in the
concentrations of alpha- and gamma-tocopherol in nervous
tissues, heart, liver and muscle of vitamin-E-deficient rats.
Biochim Biophys Acta 1334, 173-181.
[79] Morris MC, Tangney CC (2014) Dietary fat composition
and dementia risk. Neurobiol Aging 35(Suppl 2), S59-S64.
[80] McNamara RK, Liu Y, Jandacek R, Rider T, Tso P (2008)
The aging human orbitofrontal cortex: Decreasing polyun-
saturated fatty acid composition and associated increases
in lipogenic gene expression and stearoyl-CoA desaturase
activity. Prostaglandins Leukot Essent Fatty Acids 78, 293-
304.
[81] Snigdha S, Astarita G, Piomelli D, Cotman CW (2012)
Effects of diet and behavioural enrichment on free fatty acids
in the aged canine brain. Neuroscience 202, 326-333.
[82] Lebbadi M, Julien C, Phivilay A, Tremblay C, Emond V,
Kang JX, Calon F (2011) Endogenous conversion of omega-
6 into omega-3 fatty acids improves neuropathology in an
animal model of Alzheimer’s disease. J Alzheimers Dis 27,
853-869.
[83] Hashimoto M, Hossain S (2011) Neuroprotective and ame-
liorative actions of polyunsaturated fatty acids against
neuronal diseases: Beneficial effect of docosahexaenoic acid
on cognitive decline in Alzheimer’s disease. J Pharmacol
Sci 116, 150-162.
[84] Chung WL, Chen JJ, Su HM (2008) Fish oil supplemen-
tation of control and (n-3) fatty acid-deficient male rats
enhances reference and working memory performance and
increases brain regional docosahexaenoic acid levels. J Nutr
138, 1165-1171.
[85] Holguin S, Huang Y, Liu J, Wurtman R (2008) Chronic
administration of DHA and UMP improves the impaired
memory of environmentally impoverished rats. Behav Brain
Res 191, 11-16.
[86] Sakamoto T, Cansev M, Wurtman RJ (2007) Oral
supplementation with docosahexaenoic acid and uridine-5’-
monophosphate increases dendritic spine density in adult
gerbil hippocampus. Brain Res 1182, 50-59.
[87] Lim SY, Suzuki H (2002) Dose-response effect of egg-
phosphatidylcholine on maze-learning ability and fatty acid
composition of plasma and brain in aged mice fed an n-3
fatty acid-deficient diet. Ann Nutr Metab 46, 215-221.
[88] Minami M, Kimura S, Endo T, Hamaue N, Hirafuji M,
Togashi H, Matsumoto M, Yoshioka M, Saito H, Watanabe
S, Kobayashi T, Okuyama H (1997) Dietary docosa-
hexaenoic acid increases cerebral acetylcholine levels
and improves passive avoidance performance in stroke-
prone spontaneously hypertensive rats. Pharmacol Biochem
Behav 58, 1123-1129.
[89] Greenwood CE, Winocur G (1996) Cognitive impairment
in rats fed high-fat diets: A specific effect of saturated fatty-
acid intake. Behav Neurosci 110, 451-459.
[90] Puglielli L, Tanzi RE, Kovacs DM (2003) Alzheimer’s dis-
ease: The cholesterol connection. Nat Neurosci 6, 345-351.
[91] Winocur G, Greenwood CE (2005) Studies of the effects of
high fat diets on cognitive function in a rat model. Neurobiol
Aging 26(Suppl 1), 46-49.
[92] Grimm MO, Rothhaar TL, Gr¨osgen S, Burg VK,
Hundsd¨orfer B, Haupenthal VJ, Friess P, Kins S, Grimm
HS, Hartmann T (2012) Trans fatty acids enhance amyloido-
genicprocessingoftheAlzheimeramyloidprecursorprotein
(APP). J Nutr Biochem 23, 1214-1223.
[93] Oksman M, Iivonen H, Hogyes E, Amtul Z, Penke B, Leen-
ders I, Broersen L, L¨utjohann D, Hartmann T, Tanila H
(2006) Impact of different saturated fatty acid, polyun-
saturated fatty acid and cholesterol containing diets on
beta-amyloid accumulation in APP/PS1 transgenic mice.
Neurobiol Dis 23, 563-572.
[94] Sparks DL, Kuo YM, Roher A, Martin T, Lukas RJ (2000)
Alterations of Alzheimer’s disease in the cholesterol-fed
rabbit, including vascular inflammation. Preliminary obser-
vations. Ann NY Acad Sci 903, 335-344.
[95] Sparks DL, Scheff SW, Hunsaker JC 3rd, Liu H, Landers
T, Gross DR (1994) Induction of Alzheimer-like beta-
amyloid immunoreactivity in the brains of rabbits with
dietary cholesterol. Exp Neurol 126, 88-94.
[96] Takechi R, Pallebage-Gamarallage MM, Lam V, Giles C,
Mamo JC (2013) Aging-related changes in blood-brain bar-
rier integrity and the effect of dietary fat. Neurodegener Dis
12, 125-135.
[97] Morris MC, Tangney CC, Wang Y, Barnes LL, Bennett D,
Aggarwal N (2014) Mind diet score more predictive than
dash or Mediterranean diet scores. Alzheimers Dement 10
(4 Suppl), P166 (Abstract O2-02-04).
[98] Catal´a I, Ferrer I, Galofr´e E, F´abregues I (1988) Decreased
numbers of dendritic spines on cortical pyramidal neurons
in dementia. A quantitative Golgi study on biopsy samples.
Hum Neurobiol 6, 255-259.
[99] Einstein G, Buranosky R, Crain BJ (1994) Dendritic pathol-
ogy of granule cells in Alzheimer’s disease is unrelated to
neuritic plaques. J Neurosci 14, 5077-5088.
[100] Mavroudis IA, Fotiou DF, Adipepe LF, Manani MG, Njau
SD, Psaroulis D, Costa VG, Baloyannis SJ (2010) Morpho-
logical changes of the human purkinje cells and deposition
of neuritic plaques and neurofibrillary tangles on the cere-
bellar cortex of Alzheimer’s disease. Am J Alzheimers Dis
Other Demen 25, 585-591.
[101] Tsamis IK, Mytilinaios GD, Njau NS, Fotiou FD, Glaftsi S,
Costa V, Baloyannis JS (2010) Properties of CA3 dendritic
excrescences in Alzheimer’s disease. Curr Alzheimer Res 7,
84-90.
[102] Masliah E, Mallory M, Hansen L, DeTeresa R, Alford M,
Terry R (1994) Synaptic and neuritic alterations during the
progression of Alzheimer’s disease. Neurosci Lett 174, 67-
72.
[103] Scheff SW, Price DA, Schmitt FA, Mufson EJ (2006) Hip-
pocampal synaptic loss in early Alzheimer’s disease and
mild cognitive impairment. Neurobiol Aging 27, 1372-1384.
[104] Bell KF, Bennett DA, Cuello AC (2007) Paradoxical upreg-
ulation of glutamatergic presynaptic boutons during mild
cognitive impairment. J Neurosci 27, 10810-10817.
[105] Akram A, Christoffel D, Rocher AB, Bouras C, K¨ovari
E, Perl DP, Morrison JH, Herrmann FR, Haroutunian V,
Giannakopoulos P, Hof PR (2008) Stereologic estimates](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-15-2048.jpg)
![1126 D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition
of total spinophilin-immunoreactive spine number in area
9 and the CA1 field: Relationship with the progression of
Alzheimer’s disease. Neurobiol Aging 29, 1296-1307.
[106] DeKosky ST, Scheff SW (1990) Synapse loss in frontal
cortex biopsies in Alzheimer’s disease: Correlation with
cognitive severity. Ann Neurol 27, 457-464.
[107] Terry RD, Masliah E, Salmon DP, Butters N, DeTeresa R,
Hill R, Hansen LA, Katzman R (1991) Physical basis of
cognitive alterations in Alzheimer’s disease: Synapse loss
is the major correlate of cognitive impairment. Ann Neurol
30, 572-580.
[108] Kosicek M, Hecimovic S (2013) Phospholipids and
Alzheimer’s disease: Alterations, mechanisms and potential
biomarkers. Int J Mol Sci 14, 1310-1322.
[109] Mielke MM, Lyketsos CG (2006) Lipids and the pathogene-
sis of Alzheimer’s disease: Is there a link? Int Rev Psychiatry
18, 173-186.
[110] Gibellini F, Smith TK (2010) The Kennedy pathway–De
novo synthesis of phosphatidylethanolamine and phos-
phatidylcholine. IUBMB Life 62, 414-428.
[111] Wurtman RJ, Ulus IH, Cansev M, Watkins CJ, Wang
L, Marzloff G (2006) Synaptic proteins and phospho-
lipids are increased in gerbil brain by administering
uridine plus docosahexaenoic acid orally. Brain Res 1088,
83-92.
[112] Cansev M, van Wijk N, Turkyilmaz M, Orhan F, Sijben JW,
Broersen LM (2015) A specific multi-nutrient enriched diet
enhanceshippocampalcholinergictransmissioninagedrats.
Neurobiol Aging 36, 344-351.
[113] A¨id S, Vancassel S, Poum`es-Ballihaut C, Chalon S, Guesnet
P, Lavialle M (2003) Effect of a diet-induced n-3 PUFA
depletion on cholinergic parameters in the rat hippocampus.
J Lipid Res 44, 1545-1551.
[114] Lopes da Silva S, Vellas B, Elemans S, Luchsinger J,
Kamphuis P, Yaffe K, Sijben J, Groenendijk M, Stijnen T
(2014) Plasma nutrient status of patients with Alzheimer’s
disease: Systematic review and meta-analysis. Alzheimers
Dement 10, 485-502.
[115] Lin PY, Chiu CC, Huang SY, Su KP (2012) A meta-analytic
review of polyunsaturated fatty acid compositions in demen-
tia. J Clin Psychiatry 73, 1245-1254.
[116] Loef M, Schrauzer GN, Walach H (2011) Selenium and
Alzheimer’s disease: A systematic review. J Alzheimers Dis
26, 81-104.
[117] de Wilde MC, van Wijk N, Groenendijk M, Hageman R,
Kamphuis PJ, Sijben JW. (2012) Lower plasma uridine con-
centrationinpeoplewithAlzheimer’sdiseasethaninhealthy
individuals. Program No. 749.01. 2012 Neuroscience Meet-
ing Planner. Society for Neuroscience, New Orleans, LA.
[118] Trushina E, Dutta T, Persson XM, Mielke MM, Petersen
RC (2013) Identification of altered metabolic pathways
in plasma and CSF in mild cognitive impairment and
Alzheimer’s disease using metabolomics. PLoS One 8,
e63644.
[119] Olde Rikkert MG, Verhey FR, Sijben JW, Bouwman FH,
Dautzenberg PL, Lansink M, Sipers WM, van Asselt DZ,
van Hees AM, Stevens M, Vellas B, Scheltens P (2014) Dif-
ferences in nutritional status between very mild Alzheimer’s
disease patients and healthy controls. J Alzheimers Dis 41,
261-271.
[120] Wang G, Zhou Y, Huang FJ, Tang HD, Xu XH, Liu JJ,
Wang Y, Deng YL, Ren RJ, Xu W, Ma JF, Zhang YN,
Zhao AH, Chen SD, Jia W (2014) Plasma metabolite pro-
files of Alzheimer’s disease and mild cognitive impairment.
J Proteome Res 13, 2649-2658.
[121] Wurtman RJ (2014) A nutrient combination that can affect
synapse formation. Nutrients 6, 1701-1710.
[122] Czech C, Berndt P, Busch K, Schmitz O, Wiemer J, Most
V, Hampel H, Kastler J, Senn H (2012) Metabolite profil-
ing of Alzheimer’s disease cerebrospinal fluid. PLoS One 7,
e31501.
[123] de Wilde MC, Vellas B, Lopes da Silva S, Elemans S,
Swinkels S, Sijben JW, Luchsinger JA, Groenendijk M,
Yaffe K, Stijnen T (2014) Lower long-chain n-3 fatty acid
status in AD: Results from a meta-analysis. Alzheimers
Dement 10(Suppl), P674-P675.
[124] Nitsch RM, Blusztajn JK, Pittas AG, Slack BE, Growdon
JH, Wurtman RJ (1992) Evidence for a membrane defect
in Alzheimer disease brain. Proc Natl Acad Sci U S A 89,
1671-1675.
[125] Igarashi M, Ma K, Gao F, Kim HW, Rapoport SI, Rao
JS (2011) Disturbed choline plasmalogen and phospholipid
fatty acid concentrations in Alzheimer’s disease prefrontal
cortex. J Alzheimers Dis 24, 507-517.
[126] Grimm MO, Gr¨osgen S, Riemenschneider M, Tanila H,
Grimm HS, Hartmann T (2011) From brain to food: Anal-
ysis of phosphatidylcholins, lyso-phosphatidylcholins and
phosphatidylcholin-plasmalogens derivates in Alzheimer’s
disease human post mortem brains and mice model via mass
spectrometry. J Chromatogr A 1218, 7713-7722.
[127] Walter A, Korth U, Hilgert M, Hartmann J, Weichel O,
Hilgert M, Fassbender K, Schmitt A, Klein J (2004) Glyc-
erophosphocholine is elevated in cerebrospinal fluid of
Alzheimer patients. Neurobiol Aging 25, 1299-1303.
[128] Cohen BM, Renshaw PF, Stoll AL, Wurtman RJ, Yurgelun-
Todd D, Babb SM (1995) Decreased brain choline uptake
in older adults. An in vivo proton magnetic resonance spec-
troscopy study. JAMA 274, 902-907.
[129] Shatenstein B, Kergoat MJ, Reid I (2007) Poor nutrient
intakes during 1-year follow-up with community-dwelling
older adults with early-stage Alzheimer dementia compared
to cognitively intact matched controls. J Am Diet Assoc 107,
2091-2099.
[130] Phillips MA, Childs CE, Calder PC, Rogers PJ (2012)
Lower omega-3 fatty acid intake and status are associated
with poorer cognitive function in older age: A comparison
of individuals with and without cognitive impairment and
Alzheimer’s disease. Nutr Neurosci 6, 271-277.
[131] Hart K, Cave E, Conroy B, Farina N, Young J, Rusted J,
Tabet N (2013) Nutritional status of older adults with and
without dementia. Proc Nutr Soc 72 (OCE4) E247.
[132] Astarita G, Jung KM, Berchtold NC, Nguyen VQ, Gillen
DL, Head E, Cotman CW, Piomelli D (2010) Deficient
liver biosynthesis of docosahexaenoic acid correlates with
cognitive impairment in Alzheimer’s disease. PLoS One 5,
e12538.
[133] Van Dam F, Van Gool WA (2009) Hyperhomocysteinemia
and Alzheimer’s disease: A systematic review. Arch Geron-
tol Geriatr 48, 425-430.
[134] Andres E, Affenberger S, Vinzio S, Kurtz JE, Noel E,
Kaltenbach G, Maloisel F, Schlienger JL, Blickl´e JF (2005)
Food-cobalamin malabsorption in elderly patients: Clinical
manifestations and treatment. Am J Med 118, 1154-1159.
[135] Nilsson-Ehle H (1998) Age-related changes in cobalamin
(vitamin B12) handling. Implications for therapy. Drugs
Aging 12, 277-292.
[136] Carmel R (1997) Cobalamin, the stomach, and aging. Am J
Clin Nutr 66, 750-759.
[137] Refsum H, Smith AD (2003) Low vitamin B-12 status
in confirmed Alzheimer’s disease as revealed by serum](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-16-2048.jpg)
![D.R. Gustafson et al. / Alzheimer’s Disease and Nutrition 1127
holotranscobalamin. J Neurol Neurosurg Psychiatry 74,
959-961.
[138] McCaddon A, Hudson P, Abrahamsson L, Olofsson H,
Regland B (2001) Analogues, ageing and aberrant assimila-
tion of vitamin B12 in Alzheimer’s disease. Dement Geriatr
Cogn Disord 12, 133-137.
[139] de Waal H, Stam CJ, Lansbergen MM, Wieggers RL,
Kamphuis PJ, Scheltens P, Maest´u F, van Straaten EC
(2014) The effect of souvenaid on functional brain network
organisation in patients with mild Alzheimer’s disease: A
randomised controlled study. PLoS One 9, e86558.
[140] Scheltens P, Twisk JW, Blesa R, Scarpini E, von Arnim CA,
Bongers A, Harrison J, Swinkels SH, Stam CJ, de Waal H,
Wurtman RJ, Wieggers RL, Vellas B, Kamphuis PJ (2012)
Efficacy of Souvenaid in mild Alzheimer’s disease: Results
from a randomized controlled trial. J Alzheimers Dis 31,
225-236.
[141] Scheltens P, Kamphuis PJ, Verhey FR, Olde Rikkert MG,
Wurtman RJ, Wilkinson D, Twisk JW, Kurz A (2010) Effi-
cacy of a medical food in mild Alzheimer’s disease: A
randomized, controlled trial. Alzheimers Dement 6, 1-10.e1.
[142] Mapstone M, Cheema AK, Fiandaca MS, Zhong X, Mhyre
TR, MacArthur LH, Hall WJ, Fisher SG, Peterson DR,
Haley JM, Nazar MD, Rich SA, Berlau DJ, Peltz CB, Tan
MT, Kawas CH, Federoff HJ (2014) Plasma phospholipids
identify antecedent memory impairment in older adults. Nat
Med 20, 415-418.
[143] Hartmann T, van Wijk N, Wurtman RJ, Olde Rikkert
MG, Sijben JW, Soininen H, Vellas B, Scheltens P (2014)
A nutritional approach to ameliorate altered phospholipid
metabolism in Alzheimer’s disease. J Alzheimers Dis 41,
715-717.
[144] Dubois B, Feldman HH, Jacova C, Dekosky ST, Barberger-
Gateau P, Cummings J, Delacourte A, Galasko D, Gauthier
S, Jicha G, Meguro K, O’Brien J, Pasquier F, Robert P,
RossorM,SallowayS,SternY,VisserPJ,ScheltensP(2007)
Research criteria for the diagnosis of Alzheimer’s disease:
Revising the NINCDS-ADRDA criteria. Lancet Neurol 6,
734-746.
[145] Netherlands Trial Registry. LipiDiDiet Trial. http://www.
trialregister.nl/trialreg/admin/rctview.asp? TC=1705. Dec-
ember 23, 2013; Accessed September 2014.](https://image.slidesharecdn.com/newperspectivesonalzheimersdiseaseandnutrition-170711082124/75/New-Perspectives-on-Alzheimer-s-Disease-and-Nutrition-17-2048.jpg)

This document summarizes a roundtable discussion on the role of nutrition in Alzheimer's disease (AD). The discussion focused on how being overweight or obese in midlife may increase the risk of developing AD decades later, though evidence is conflicting. After midlife, higher body weight and BMI are associated with lower dementia risk. Weight loss and underweight in late life are linked to higher dementia risk. The natural trajectory of BMI over the lifespan differs between those who do and do not develop dementia. Changes in BMI and weight loss may also be associated with clinical progression of AD. Further research is needed to better understand these complex relationships between nutritional status and AD risk and progression.









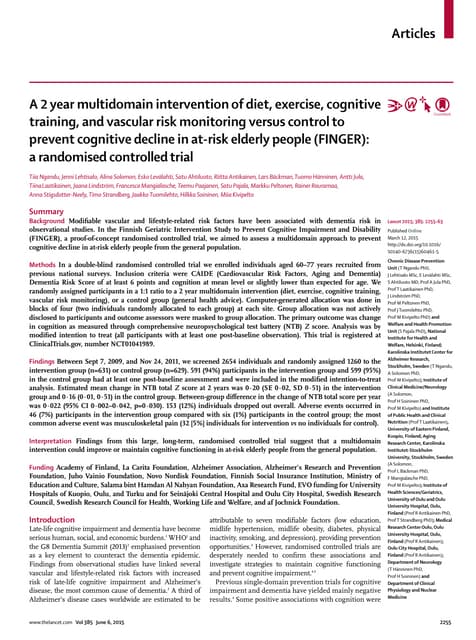

![Journal club: long-term cognitive impairment after critical illness [NEJM 369]](https://cdn.slidesharecdn.com/ss_thumbnails/slides-150429113717-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)





















































