Being able to prognosticate in the aftermath of a traumatic brain injury (TBI) is important as it assists with counselling patients and families. Moreover, it helps rationally allocate healthcare resources.
However, due to the heterogenous nature of TBI and variable pre brain injury patient factors and post brain injury course, this has proven to be a difficult task.
Large cohort studies have enabled improved accuracy in the prediction of 6 month mortality and unfavourable outcome.
Furthermore, many of the factors that contribute to long-term outcome have also emerged. However, it is not yet possible to use them in prediction algorithms or mathematical models.
There is emerging evidence that pre injury psychosocial and demographic factors may be of more relevance than injury severity. Moreover, that 'outcome' becomes increasingly subjective and complex as the post injury duration increases.
We end with three brief vignettes which highlight the fraught nature of long term outcome prediction.
Epilepsy can occur after stroke, and is more common in elderly population. This talk looks at classification, epidemiology, pathogenesis, clinical presentation and treatment of post-stroke seizures and epilepsy. The risk factors for the development of post-stroke seizures have also been looked at.
ABSTRACT
care in Pediatric head injuries –Nursing Neuro surgery ICU
Anu Antony , Deepak Agrawal
Department of Neurosurgery, JPNA Trauma Centre, AIIMS ,New Delhi
Background: Nursing assessment of pediatric head injuries is difficult as GCS scoring system is not applicable to this age group. Also managing head injured children in the same ICU with adults is challenging
Objectives: To assess outcome of admitted pediatric head injury patients (<12yrs) as a surrogate marker for nursing care in the ICU.
Materials &methods: In this prospective study over 9months (Jan2011-Sept2011), the demographic profile ,surgical intervention ,mode of injury and outcome was evaluated for all children with head injury admitted in neurosurgery ICU at JPNA Trauma Center AIIMS.
Result: 104 children with head injury were admitted in the ICU during study period. There were 70males & 34 females. The mean age was 6.5yrs (range day1-12yrs) 51 children had severe head injury, 19 had moderate&34had minor head injury. 51(49%) children underwent surgical intervention. The overall mortality rate was 19.23%(n-20).Mortality rate was 33.3% (n-17) in severe head injuries,5.9% (n-2) in minor head injuries and 5.2%(n-1) in moderate head injury group.84 children were discharged .Of these 84.5%(n-71)had improvement in GCS,10.7%(n-9) had same GCS&4(4.7%) children deteriorated. The average hospital stay was 10 days (range2-94 days).2 patients were still hospitalized at the time of this study.
Conclusion: The mortality rates compare very favorably with international data. This study shows head inured children can be managed appropriately in neurosurgery ICU with nurses trained in neuro- nursing
Brain tumor is one of the leading cause of mortality and morbidity among human beings. In this chapter, fundamental principles, concepts related to brain tumors and related management are explored. Nurses provide sensitive, supportive care to the patient and family.
Being able to prognosticate in the aftermath of a traumatic brain injury (TBI) is important as it assists with counselling patients and families. Moreover, it helps rationally allocate healthcare resources.
However, due to the heterogenous nature of TBI and variable pre brain injury patient factors and post brain injury course, this has proven to be a difficult task.
Large cohort studies have enabled improved accuracy in the prediction of 6 month mortality and unfavourable outcome.
Furthermore, many of the factors that contribute to long-term outcome have also emerged. However, it is not yet possible to use them in prediction algorithms or mathematical models.
There is emerging evidence that pre injury psychosocial and demographic factors may be of more relevance than injury severity. Moreover, that 'outcome' becomes increasingly subjective and complex as the post injury duration increases.
We end with three brief vignettes which highlight the fraught nature of long term outcome prediction.
Epilepsy can occur after stroke, and is more common in elderly population. This talk looks at classification, epidemiology, pathogenesis, clinical presentation and treatment of post-stroke seizures and epilepsy. The risk factors for the development of post-stroke seizures have also been looked at.
ABSTRACT
care in Pediatric head injuries –Nursing Neuro surgery ICU
Anu Antony , Deepak Agrawal
Department of Neurosurgery, JPNA Trauma Centre, AIIMS ,New Delhi
Background: Nursing assessment of pediatric head injuries is difficult as GCS scoring system is not applicable to this age group. Also managing head injured children in the same ICU with adults is challenging
Objectives: To assess outcome of admitted pediatric head injury patients (<12yrs) as a surrogate marker for nursing care in the ICU.
Materials &methods: In this prospective study over 9months (Jan2011-Sept2011), the demographic profile ,surgical intervention ,mode of injury and outcome was evaluated for all children with head injury admitted in neurosurgery ICU at JPNA Trauma Center AIIMS.
Result: 104 children with head injury were admitted in the ICU during study period. There were 70males & 34 females. The mean age was 6.5yrs (range day1-12yrs) 51 children had severe head injury, 19 had moderate&34had minor head injury. 51(49%) children underwent surgical intervention. The overall mortality rate was 19.23%(n-20).Mortality rate was 33.3% (n-17) in severe head injuries,5.9% (n-2) in minor head injuries and 5.2%(n-1) in moderate head injury group.84 children were discharged .Of these 84.5%(n-71)had improvement in GCS,10.7%(n-9) had same GCS&4(4.7%) children deteriorated. The average hospital stay was 10 days (range2-94 days).2 patients were still hospitalized at the time of this study.
Conclusion: The mortality rates compare very favorably with international data. This study shows head inured children can be managed appropriately in neurosurgery ICU with nurses trained in neuro- nursing
Brain tumor is one of the leading cause of mortality and morbidity among human beings. In this chapter, fundamental principles, concepts related to brain tumors and related management are explored. Nurses provide sensitive, supportive care to the patient and family.
you will learn about brain tumor, types of brain tumor, grading of brain tumor, risk factors for brain tumor, diagnosis for brain tumor, treatment for brain tumor, supportive care and rehabilitation for patients with brain tumor.
Very beggining of my post graduation journey I prepared it for weekly presentation in my oncology department RAJSHAHI MEDICAL COLLEGE. sharing here if anyone get any help who r begginer in this field. Thank you.
O artigo fala sobre a reabilitação em pacientes com tumores cerebrais sob uma visão multidisciplinar, visando a funcionalidade e tratamento das sequelas.
Management of Brain Tumors in Pediatric Age Group.pptxssuser903c9d
The presentation titled "Management of Brain Tumors" focuses on pediatric neurosurgery approach on addressing brain tumors in children. The presentation dives into the background of brain tumors, detailing their prevalence, types, and distribution among children, and compares these aspects with adult cases. It outlines the symptoms, diagnostic approaches, and treatment options including surgery, radiation therapy, and chemotherapy. The presentation also discusses specific tumor types, prognostic factors, and the importance of supportive care and rehabilitation. It concludes with a summation on the significance of addressing pediatric brain tumors at the earliest.
Neuroblastoma is the most common cancer in babies and the third-most common cancer in children after leukemia and brain cancer, proper diagnosis, treatment must be done in appropriate time. As it a fatal condition psychosocial support is most important for patient and family.
A review of epilepsy in the elderly, the etiopathogenesis, clinical challenges, diagnosis, use of antiseizure drugs and outcomes. Also the various special considerations in managing elderly patients with epilepsy.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Neurosurgeon in Mumbai: DR Vinod Rambal at Dr L H Hiranandani Hospital, Mumbai
1. HealthyLifeN e w s l e t t e rIssue-06 | April 2010 www.hiranandanihospital.org
Brain Tumors ............................................1
Injuries... ................................................. 2
Epilepsy.....................................................3
Parkinson's Disease ................................ 4
Lumbar Disc Prolapse ............................. 4
Diagnostic Neuroradiology ...................... 5
Department of Neurosciences
CALL US FOR ANY QUERY: + 91-22-2576 3300
Winner of IMC Ramkrishna Bajaj National Quality 2008 &Award - International Asia Pacific Quality Award (IAPQA) - 2009
Mumbai's First NABH Accredited Hospital
The annual incidence of brain tumors is 22 per symptoms like headache, convulsions or
1,00,000 persons. Incidence of tumor varies vomiting. These tumors need to be removed.
with age. There is a small peak at 2 years, a Surgery provides the confirmation, helps in
decline for the rest of the first decade and slow alleviation of the symptoms and facilitates
increase from 2 per million at age 20 to 6 per future planning and treatment. Depending on
million at age 40. About half of them are primary the grade of the tumor, further adjuvant therapy
and rest are metastatic in origin. can be offered. The options are radiotherapy,
chemotherapy, immunotherapy, biologicalThere are two main groups of tumors, which
response modifiers and inhibitors ofare quite diverse in their origin, behaviour and
angiogenesis. Lower grades, where oneoutcome.
achieves a gross total removal, have a good
In benign category, the biggest challenge is to outcome in terms of survival and quality of life.
remove the tumor completely and to safeguard Lower grades have a 5-year survival of around
the adjacent normal brain. These tumors arise 80%. High-grade tumors especially grade IV,
outside brain parenchyma or neighbouring survival is less than a year with best possible
skull base and insinuate into the normal brain. treatment, surgery plus adjuvant.
These are slow growing and keep pushing or
Malignant tumors from lung, breast, prostrate,displacing normal brain. Usual presentation is
colorectal, kidney and melanoma commonlythat of general symptoms of headache, raised
spread to the brain. It usually occurs at grey-intracranial pressure features, convulsions in
white junction, however, it can grow atsupratentorial tumors or obstructive
anywhere in the brain. About 15% may presenthydrocephalus in infratentorial tumors.
as an occult primary. Treatment recommended
Malignant tumors usually arise from the is surgery in solitary metastasis, followed by
supporting glial cells of neural tissue. These whole brain radiation or Stereotactic
tumors being intrinsic in nature manifest by way Radiosurgery.
of either 'area-located' symptoms or general
BRAIN TUMORS
Dr Vinod Rambal
MS, MCh (Neurosurgery)
Full-time Consultant Neurosurgeon
A 62 year old male with Oligodendroglioma
A 60 year old female with Meningioma(H & E, 100X)
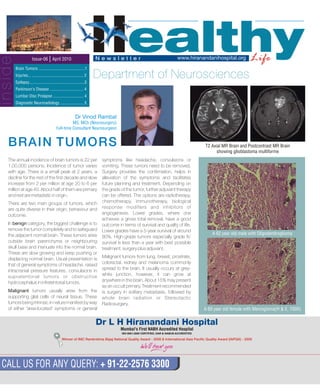
T2 Axial MR Brain and Postcontrast MR Brain
showing glioblastoma multiforme
inside
2. INJURIES WITH
NEUROLOGICAL AFTER-EFFECTS
Dr Vinod Rambal
MS, MCh (Neurosurgery)
Full-time Consultant Neurosurgeon
Cervical spine being the most mobile portion of the spine is
vulnerable and is a common site of injury. Major causes are
motor vehicular accidents, accidental falls and sports
associated injuries. The cause varies with age and sex;
males being 3 to 4 times more common than females. The
most frequent age group to suffer a spinal cord injury is 15-
30 years. Spinal cord injury is unfortunately very common
and occurs in 40-60% of patients.
Injuries can be bony, ligamentous or combination of both.
External immobilisation is a must, at site / pre-hospital,
much before any definitive treatment is planned. The spinal
injuries may be in isolation or in association with head
injuries. Identifying the other areas involved needs imaging
(such as MRI, X-rays and ultrasound) and examining the
other organ injuries entails risk to the existing spinal cord
injury. Any body movement may enhance or worsen the
existing spinal cord damage, especially when vertebral
column is broken.
X-ray showing cervical vertebrae fracture
The broken vertebral column needs to be stabilised initially
from outside and subsequently from within. Depending on
the area involved, there may be cardiovascular or
autonomic disturbances associated which will merit special
attention and treatment. The associated bladder and bowel
care needs to be instituted.
It usually involves younger age group, in their fruitful years of life. High-speed
motor vehicular accidents are common; other causes are home and
occupational accidents, accidental falls and assaults. It includes both,
injuries to brain and parts of the head, such as scalp and skull. Specific
problems after head injury can include - skull fracture, laceration to the
scalp, traumatic subdural and extradural haematoma, traumatic
subarachnoid haemorrhage and cerebral contusion.
In closed head injury cases, prompt cardiorespiratory stabilisation and
clinical neurological examination is a must. Once that is achieved, patient is
intubated, sedated and mechanically ventilated to restore blood pressure,
oxygenation and ventilation. CT scan of the brain allows us to decide further
management. In cases of extra or subdural haematomas, quick surgical
evacuation is helpful. Diffuse injuries and contusions need to be
aggressively handled. One needs to manage intracranial pressure surges.
Uncontrolled raised pressure increases the morbidity and mortality.
Monitoring intracranial pressure is most rewarding. Various medical options
are available apart from surgical intervention. Ventilation, maintaining
normocapnia, 3% saline infusion helps to combat raised intracranial
pressure. Glasgow coma scale (GSC) helps in predicting the outcome. The
GSC score of 14-15 is mild injury; moderate, when the score is 9-13 and
severe injury, score is 8 or less. Hypotension and hypoxia greatly increase
the morbidity and mortality. In case there are other organ involvement,
screening those suspected areas is a must. Haemoglobin should be
maintained in the normal range. Surgery encompasses a wide range of
procedures, which will be dictated by clinical picture and CT scan findings
and response to the conservative medicines. The basic issue of raised
intracranial pressure needs to be ameliorated. It is the global ischaemia
secondary to raised intracranial pressure due to diffuse cytotoxic and
vasogenic oedema, which induces further damage and determines the
ultimate outcome. Severe head injury patients have associated injuries, the
incidence being long bone fractures-32%, Maxillary / mandibular fractures-
22%, major chest injury-23%, abdominal visceral injury-7% and spinal injury
in about 2% of patients.
CT scan showing head injury
HEAD INJURY
CT scan showing cervical spine injury
CERVICAL SPINE INJURY
3. Epilepsy is defined as a disorder of brain and brain tumors. At times, metabolic disturbance Choice of Anti-epileptic Therapy in Chronic
characterized by an ongoing liability for recurrent in body may induce seizure. Active Epilepsy
epileptic seizures. Seizure (from the latin word There is a choice from newer anti-epileptic drugsClassification and Diagnosis
'sacire' meaning “to take possession of”) is a like Levitracetam, Zonisamide, Topiramate,The International League against Epilepsy (ILAE)
paroxysmal event due to abnormal, excessive, Clobazam, Oxcarbamazepine, Gabapentin etc.has outlined a broad and comprehensive
hypersynchronous discharge from an aggregate of
classification. Broadly, epilepsy can be classified Drug choice may change with specific patient
central nervous system neurons. However, the
as partial-onset involving focal brain areas and groups like elderly, pregnant women etc
manifestation of such activity may differ from
involving unilateral body parts and generalized Adverse effect profiles differ and should beperson to person and manifest iteslf present in
due to diffuse brain involvement. Diagnosis of taken into account and may vary with individualvaried forms.Two or more unprovoked seizures are
epilepsy requires a detailed history and ruling out patientknown as epilepsy.
non-epileptic attacks like syncope, Transient
Monotherapy will be useful in about 70-80% of Incidence is about 80 new cases in every Ischemic Attacks (TIA) and psychogenic non-
cases and should be chosen whenever1,00,000 persons per year epileptic attacks. EEG helps in localizing epilepsies
possiblethough a normal EEG does not rule out seizures. Prevalence is about 4-10 cases per 1000
Neuroimaging helps to find out structural brain Combination anti-epileptic drugs may bepersons
lesions, cyst, brain tumors etc. needed in about 20-30% cases, more in
Overall prevalence of epilepsy in India is 5.33
cases which have remained uncontrolledTreatmentper 1000 persons
in spite of initial Monotherapy
The approach to drug treatment for epilepsy It occurs in all parts of the world and in all strata
Discontinuation of anti-epileptic drugs shouldbroadly depends on:of population
be gradual and the decision is made by a
1. Seizure type About 40% of cases of epilepsy occur below 16 specialist on case-to-case basis
years of age and 20% occur above 65 years of 2. Stages Newly diagnosed, Chronic epilepsy, Ketogenic diet is an alternative therapy for
age Epilepsy in remission children who have difficult-to-control epilepsy.
Cumulative incidence of epilepsy - the risk of This diet is a high fat, adequate protein, very low3. Epilepsy syndrome
an individual having a seizure in their lifetime is carbohydrate diet which is carefully and
4. Special patient groups
about 4% individually calculated for each child
Initial Antiepileptic Drug in Drug-naïve
What is the cause?
Cases
Cause of epilepsy may vary in different age groups.
1. Generalized Tonic-clonic Seizures
In newborn, they can be due to birth-asphyxia,
Valproateinborn errors of metabolism and deficiency states
Phenytoin, Lamotrigine and Carbamazepinelike hypocalcemia and pyridoxine deficiency.
are alternative drugs
In children, they can be due to CNS infections and
Phenobarbital
more commonly seen in a syndrome known as
2. Partial-onset Epilepsy'febrile convulsions'. This condition is usually
Carbamazepine is drug of choicebenign.
Valproate, Phenytoin, Oxcarbamazepine andIn adolescents and early adulthood, a common
Lamotrigine are alternativescause of epilepsy is 'Juvenile Myoclonic Epilepsy'
(JME) where generalized tonic-clonic seizures are 3. Myoclonic Epilepsy
associated with myoclonic jerks and at times Valproate
absence seizures. These seizures belong to a Lamotrigine or Clonazepam may be used as
Surgery in epilepsy may be required in refractorygroup known as 'Idiopathic Generalized Epilepsy'. alternatives
epilepsy with a structural brain lesion such asIn India, infections such as neurocysticercosis
4. Absence Epilepsy Neuronal Migrational Disorder, Mesial Temporaloccur commonly due to ingestion of tapeworm,
Valproate or Ethosuximide Lobe Sclerosis (MTLE), Ganglioneuroma, BrainTaenia solium, and tubercular abscess.
Tumors etc.
In adults and elderly, epilepsy can be due to stroke
EPILEPSY
Dr Gautam Tripathy
MD, DM (Neurology)
Full Time Consultant Neurologist
4. LUMBAR DISC PROLAPSE –
CHRONIC PAIN IN THE BACK
Dr Vinod Rambal
MS, MCh (Neurosurgery)
Full-time Consultant Neurosurgeon
It is estimated that 50% of working adults will intervention. Surgery helps them to get back to
experience back pain in any given year. normal life quickly. Frequent relapses result in the
Neurosurgeons have extensive training in the cascade of events and ultimately result in canal
management of disorders of the brain and stenosis. Currently surgical options are 'keyhole
peripheral nervous system. The syndromes microsurgical procedures'. The 'conventional
produced due to lumbar disc herniation include laminectomy' has no role in disc pathology.
radiculopathy, neurogenic claudication and cauda Laminectomy means removing posterior bony
equine syndrome. elements, resulting in spinal instability. With
microsurgical procedures, the individual is pain-Majority of patients will settle on conservative
free, active and back to work in a fortnight. Posture-treatment. Those who do not settle with
correction and muscle strengthening is required toconservative treatment will need surgical
stay fit.
Lumbar disc prolapse
Clinically, patient with the Parkinson's disease has stress. This in turn may be due to environmental
at least two out of three cardinal features of tremor, factors, toxin exposure, genetic factors or an
rigidity and bradykinesia. Postural instability may interaction between these factors. Environmental
appear late. In case it appears early, other toxins implicated include MPTP (Methyl-phenyl-
diagnosis closely related to Parkinson's disease tetrahydropyridine). Several lines of evidence point
known as 'Parkinson's Plus syndrome' should be to hereditary factors in Parkinson's disease and
considered. Patients with Parkinson's disease PARK gene mutation has been implicated in them.
have a good clinical response to Levodopa. Treatment options include MAO-B inhibitors like
Prevalence rates are about 10-400 cases per Selegiline and Rasagiline can be used as initial
1,00,000 people. There is no significant difference monotherapy and as adjunct therapy to levodopa.
between male and female. The Parsi community of Selegiline was the subject of a major
Mumbai has a prevalence of Parkinson's disease neuroprotective trial in Parkinson's disease. Early such cases includes addition of Dopamine agonist
of 328.3 per 1,00,000. India, as a whole, has a low symptomatic therapy can be chosen from an array and COMT Inhibitors. Surgery in Parkinson's
prevalence. of drugs though Levodopa remains the mainstay of disease is used for fluctuating symptoms and
therapy. Dopa-agonists like Ropirinole,The usual age of onset is after 50 years with the severe Dyskinesia. Functional surgery using Deep
Pramepixole, and Amantadine may also be used.frequency rising steeply with age. Onset before 40 Brain Stimulation (DBS) device interrupts output
COMT inhibitor Entacapone prolongs the half-lifeyears is unusual and before 20 years is from sub-thalamic nucleus and globus pallidus
of Levodopa.exceptional. The cause of Parkinson's disease is pars interna. At present, the procedure is used only
the destruction of pigmented dopaminergic Anticholinergics are useful in tremors. Patients on for patients whose symptoms cannot be
neurons of the substantia nigra and some other long-term Levodopa therapy may develop adequately controlled with medications or those
brain regions. The mechanism appears to involve treatment-related complications like Dyskinesia who have medications associated with severe side
defective mitochondrial respiration and oxidative and 'off-on' phenomenon. Treatment option in effects like dyskinesia.
“Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
when supported,
with propensity to bend the trunk forward and to pass from walking to running pace;
the senses and intellects being uninjured.”
James Parkinson's original description of this disorder immediately suggests one of the most
distinctive conditions of neurology.
PARKINSON'S DISEASE
Dr Gautam Tripathy
MD, DM (Neurology)
Full Time Consultant Neurologist
5. DIAGNOSTIC
NEURORADIOLOGY-
An OVERVIEW
Dr Anand Gupta
DNB (Radiology), DMRD
Consultant Radiologist and Specialist in MRI / CT
Neuroimaging includes use of various techniques to directly or indirectly
image the structure and function of the brain and spinal cord / nerves.
tumor, demyelination, epilepsy, metabolicIMAGING MODALITIES AND THEIR
disease, congenital anomaly andSIGNIFICANCE
neurodegenerative disease.Diagnostic Imaging procedure of the
nervous system includes Myelography, MRI Diffusion-Weighted Imaging (DWI)
Computed Tomography (CT) and Magnetic is a novel technique, which is sensitive to
Resonance Imaging (MRI). increase in restriction to water diffusion, as
Advanced diagnostic modalities include a result of Cytotoxic Edema. Following an
dynamic CT angiography and MR ischemic stroke, DWI is highly sensitive to
angiography, Perfusion CT and MRI, and the changes occurring in the lesion.
Functional Magnetic Resonance Imaging Coupled with imaging of cerebral
(fMRI). perfusion, researchers can highlight
regions of 'perfusion / diffusion mismatch'CT scanner uses a series of x-rays taken
that may indicate regions capable offrom many different directions, which are
salvage by reperfusion therapy.interpolated. It is an extremely fast
technique and is a first line investigation in Diffusion Tensor Imaging (DTI) enables
head injury and strokes. researchers to make brain maps of fiber
directions to examine the connectivity ofRecent development of multi-slice
different regions in the brain (usingscanners has enabled multi-planar imaging
Tractography) or to examine areas of neuralwith extremely robust CT Angiography
degeneration and Demyelination incomparable to diagnostic accuracy of
diseases like Multiple Sclerosis.Digital Substraction Angiography (DSA)
which is an invasive study. Magnetic Resonance Spectroscopy
Magnetic Resonance Imaging (MRI) (MRS) is used to measure the levels of
uses a powerful magnetic field to align the different metabolites in body tissues. This
nuclear magnetization of (usually) hydrogen signature is used to diagnose certain
atoms in water in the body. MRI provides metabolic disorders, differentiate between
much greater contrast between the different space-occupying lesions and
different soft tissues of the body than CT, provide information on tumor metabolism.
making it especially useful in acute stroke,
CTA showing
large intracranial aneurysm
Chiari 1 malformation Multiple Myeloma in Spine
Latest MR at Dr L H Hiranandani Hospital
6. Dr L H Hiranandani Hospital
Hillside Avenue, Hiranandani Gardens, Powai,
Mumbai - 400 076.
Tel: 2576 3300 / 3333 Fax: 2576 3344 / 3311•
Hiranandani Hospital
‘ ’Hamilton B , Hiranandani Estate,
Off. Ghodbunder Road, Patlipada, Thane (W) - 400 607.
E-mail: info@hiranandanihospital.org
• Dr Sujit Chatterjee
• Dr Suvin Shetty
• Mr Manish Joshi
• Ms Debashree Sanyal
Editorial Team
Contact Us
E-mail: wecare@hiranandanihospital.org • homecare@hiranandanihospital.org
pathologyuser@hiranandanihospital.org
Board (Powai) : 2576 3300, 2576 3333, 2576 3999
Multitask Counter : 2576 3485, 2576 3486
Casualty : 2576 3322, 2576 3323, 2576 3328, 2576 3271
Laboratory : 2576 3366, 2576 3365, 2576 3234
Home Health Care : 2576 3322, 98198 73621
Ambulance : 2576 3328, 2576 3323
Health-check : 2576 3318, 2576 3398
Blood Bank : 2576 3355, 2576 3356
OPD Counter : 2576 3337, 2576 3338, 2576 3339, 2576 3340
Centralised OPD Appointment : 2576 3500
Hiranandani Hospital, Thane : 2545 8666, 2530 8666, 2530 8670, 2530 8668
A man went to the doctor. The doctor came in and said, "Well, I have got some good news and some bad
news. The bad news is that you have an inoperable brain tumor. The good news is our hospital has just
been certified to do brain transplants and there has been an accident right out front and a young couple
was killed and you can have which ever brain you like. The man`s brain is Rs. 100,000.00 and the
woman's brain is Rs. 30,000.00. The patient could not help but ask, "Why such a large difference
between the male and the female brain?" The doctor replied, "The female brain is used."
"
Magnetic Resonance Angiography
(MRA) can be performed non-invasively and
provide excellent images of the vascular tree
to evaluate them for Stenosis or Aneurysms.
MRA is often used to evaluate the arteries of
the neck and brain with variety of techniques
including use of a paramagnetic contrast
agent (Gadolinium) which provides DSA-like
images.
Magnetic Resonance Gated Intracranial
Cerebrospinal Fluid (CSF) flow study is a
method for analyzing CSF circulatory
system dynamics in patients with CSF
obstructive lesions such as normal pressure
hydrocephalus. It also allows visualization of
both arterial and venous pulsatile blood flow
in vessels without use of contrast agents.
Functional Magnetic Resonance
Imaging (fMRI) relies on the paramagnetic
p r o p e r t i e s o f o x y g e n a t e d a n d
deoxygenated hemoglobin to see images of
changing blood flow in the brain associated
with neural activity. This allows images to be
generated that reflect which brain structures
are activated (and how) during performance
of different tasks.
Large lipid / lactate peak in Tuberculoma
Middle cerebral artery
territory acute infarct
Tumor Perfusion Time of Flight (TOF) Angiogram
showing Multiple Intracranial Aneurysms
MRV showing right transverse and
sigmoid sinus thrombosis