Hx & P/E
C/C- Irritability /3 Days & failure to suck /1 day
Patient is born from a 27yrs old para III Lady whose LMP was
on 28/2/00 making GA by date 40wks+3d.Mother had a
regularANC follow up, Blood group UK,VDRL-NR, &
claims to be non reactive for HIV.
Labor started spontaneously & lasted for 5hrs; ROM was just
before delivery & the outcome was an alive male neonate who
cried immediately. Delivery was attended at home (mother
was alone) & neonate was left on the ground(soil) for
~30’before his umblicus is cut, which was done after boiling a
new lancet.
3.
Hx cotd.
Neonatewas relatively healthy sucking well until 9 days of
age when he started to become irritable followed by
decreased sucking after a day.
On the 3rd
day patient completely failed to open his mouth &
suck; he had also frequent twitching of the exterimities
Despite the ANC ffup mother didn’t receive any vaccination
in the current or previous pregnancies despite medical
advice.
Mother denied any application of herbal medication or butter
on the umblicus
4.
Hx contd.
There’sno maternal Hx of fever or foul smelling vaginal
discharge.
No maternal Hx of HTN or DM.
Mother is illiterate, Father learnt up to grade 8.
Mother is a daily laborer & father is a weaver & earn ~800
birr/month.
5.
P/E
Wt-3000gms, Length-43cm,HC-35-5cm
AHR-140’ , RR-78’ , Temp.-37 C
HEENT- Pink conjuctiva ,NIS ;Locked jaw
CHEST- has IC & SC retraction,clear
CVS- S1 & S2 well heard ,no murmur or gallop
ABD.- Rigid abdomen, difficult to palpate for organomegally
GUS.- NMEG
EXT – no edema
CNS- Conscious; Moro- Incomplete, Grasp-strong ,Tone -
increased: Sucking – sustained but difficult to open the jaw
6.
Hx & P/EContd.
Assessment –Term, LONS ?Meningitis , N.Tetanus
Plan- CBC,LP,RBS
-Start Crystalline Penicillin(333,333IU/kg/d) &
Gentamycin (5mg/kg/d)
-Diazepam 1.5mg iv bid (1mg/kg/d) alternated with
-CPZ 1.5mg iv bid (1mg/kg/d)
-TAT 5000IU IV & IM 6000IU
-Intranasal Oxygen & kept NPO
-Put under a dark cabin
COURSE & MANAGEMENT
ON23/11/00 Eth.C.
P-NeonatalTetanus
LONS? Meningitis
-On iv Crystalline & Gentamycin
-On IV Diazepam & CPZ
O- PR-162’ RR-86’ Temp- 37.6c
HEENT- Pink conjuctiva, NIS: Edematous eyelids; mild trismus
CHEST- Flaring, IC/SC retractions;clear
CVS- no murmur or gallop
ABD. - mild rigidity
CNS - Irritable
ASS. - Fair
PLAN- Continue with the same management; observe for spasms.
9.
Course contd
ON 24/11/00
Diazepam was discontinued b/c of resp. embarassment & was
made to continue CPZ only; but mother couldn’t afford anything &
patient was on IV antibiotics only.
ON 28/11/00
P- N.Tetanus
On IV Antibiotics
S- Frequent spasm, periorbital swelling, Sweating
O-V/S- AHR-124’ RR-64’regular Temp—
HEENT- Periorbital swelling with discharge
CHEST- Clear
10.
Course contd
ABD.-Rigidabdomen
EXT- increased tone
CNS- Conscious, spasms witnessed
ASS.- same, + ?sepsis with meningitis+ conjuctivitis
PLAN- Resume CPZ & Diazepam; continue antibiotics ;TTC
eye ointement
Mother couldn’t get the CPZ & was put on Diazepam only
Course contd
ON 26/12/00
P-N.Tetanus, HAS
On iv ceftriaxone & cloxacillin; iv diazepam
S-No complaint except for sweating
O-AHR-124’ RR-56’ Temp-afeb
HEENT-Pink conj.NIS
CHEST-Clear
ABD-No organomegally, mildly tense
CNS-Conscious & intact reflexes
ASS- Improved
PLAN- Discharge with advice on vaccination& po diazepam.
15.
NEONATAL TETANUS
Causedby a spore forming obligate, gram positive anaerobe
which is present in the soil, dust,& alimentary tracts of many
animals.
In developing countries approximately 1,000,000 cases of
tetanus are estimated to occur worldwide each year
Neonatal tetanus, which theWHO originally targeted for
elimination by 1995, accounted for 200,000 deaths in the year
2000 ( 200,000-500,000 deaths /year)
In Ethiopia ,a community based study conducted in Southern
Ethiopia(1989) ,estimated MR of neonatal tetanus
6.7deaths /1000 live births ; or 40% of all neonatal deaths.
16.
PATHOGENESIS
In anewborn, the portal of entry of the bacilli is almost
always the site at which the umbilical cord is cut .
After inoculation C. tetani can then transform into a
vegetative rod-shaped bacterium and produces toxins called
tetanospasmin & tetanolysin.
Through retrograde axonal transport ,it reaches the SC &
brainstem where it binds tightly and irreversibly to receptors
(inhibitory interneurons) & thus blocks neurotransmission
by its cleaving action on membrane proteins involved in
neuroexocytosis (i.e. prevents release of GABA)
17.
Pathogenesis contd.
Lackof neural control of adrenal release of catecholamines
induced by tetanospasmin produces a hyper sympathetic state
that manifests as sweating, tachycardia and hypertension.
Recovery requires the growth of new axonal nerve
terminals, thus the usual duration of clinical tetanus is four
to six weeks.
TRANSMISSION - occurs through infection during
unhygienic cutting of the umbilical cord or improper handling
of the cord stump;
It’s the only vaccine preventable Ds that’s not
communicable.
18.
CLINICAL FEATURES
Differenttypes
Generalized (the most common)
Localized
Cephalic in older children
Incubation Period - the time between the start of infection
and the occurrence of the first symptom, usually
trismus (lockjaw).
Ranges from 3-28 days; but usually lasts 2-14 days
Period of Onset - time from 1st
symptom to
occurrence of spasms; important for prognosis.
19.
C/F CONTD.
Asa rule, neonatal tetanus follows a
descending pattern of nerve
involvement
Failure to suckle is often the first sign of
infection , followed by difficulty swallowing,
stiffness in the neck, rigidity of abdominal
muscles, and a temperature rise of 2ºC –
4ºC above normal.
C/F CONTD.
•Rigidity
•+/- Infectedstump
ABD
•Dysuria, urinary retention
•Forced defecation, myoglobinuria, sometimes
RF
GUS
•Opistotonus ,Fractures,
•Bleeding into muscle
MSS
22.
C/F CONTD.
• Conscious& in extreme pain
• irritability, restlessness
CNS
•Fever, sweating
Others
•Spasms peak in the 1st
1wk after onset, stabilize
in the 2nd
wk & lessons in the following 1-
4wks.
Spasms
23.
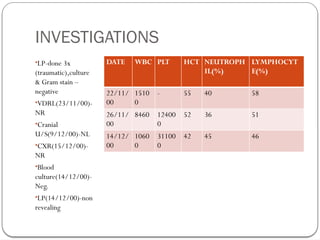
DIAGNOSIS
Clinical
Labinvestigations –
• WBC- NL OR Increased if there is
superinfection
• -LP- Non revealing
• Gram stain- positive in only 1/3rd
of the cases
• EEG & Electromyogram - Normal
24.
CASE DEFINITIONS
SuspectedCase
Any infant with a history of tetanus-compatible illness during the first month of life
who fed and cried normally for the first 2 days of life;
Any neonatal death in a child who could suck and cry normally during
the first 48 hours of life.
Confirmed Case
Normal feeding and crying during the first two days of life
plus
Onset of illness between age 3 and 28 days plus
Inability to suckle (trismus), followed by stiffness (generalized
muscle rigidity) and/or convulsions (muscle spasms).
25.
CASE DEFINITIONS CONTD.
Discarded case
A discarded case is one which has been
investigated and does not satisfy the
clinical criteria for confirmation.
MANAGEMENT
The goals oftreatment include:
Halting the toxin production
Neutralization of the unbound toxin
Control of muscle spasms
General supportive management
Prevention
28.
Management contd.
A. HaltingToxin Production
Wound debridement - to eradicate spores and necrotic tissue
Antimicrobial therapy -
Penicillin G (100,000IU/kg/day) for 10-14 days
OR
Metronidazole (30 mg/kg/day, given at six hour
intervals; maximum 4 g/day) ; currently more
recommended than the penicillins which have a
GABA antagonistic effect.
29.
Management contd.
B. Neutralizationof the unbound toxin
TIG- Doses as small as 500IU is sufficient to neutralize the
unbound toxin as soon as possible.
TAT- 10,000IU ,Given as ½ IM & ½ IV
C. Control of Muscle Spasms
o Admit to a quiet, darkened room where all possible auditory,
visual, tactile, or other stimuli are minimized
o Sedatives- Diazepam (0.1-0.2mg/kg upto 2-6wks); CPZ,
Dantrolene can be used;
o Neuromuscular Blocking Agents – Pancuronium( though it
exacerbates autonomic instability) ; Vecuronium- given as a
continious infusion can be used but with mechanical ventilation.
30.
Management contd.
D .General supportive care
Use of High Calorie diet,TPN if possible or vigourous
support through NGT
Frequent change of position esp. after spasms have decreased
Preparation for possible tracheostomy
Frequent Cardio respiratory monitoring, continuous
suctioning
Use of antacids or H2 blockers to prevent GI hemorrhage
Nursing care to the mouth ,skin, bladder
31.
COMPLICATIONS
Aspiration pneumonia,
Pneumothorax & pneumomediastinum if pt was
intubated;
Cardiac arrythmias,Asystole
Tongue bite, fractures, bleeding into muscles &
myoglobinuria leading to Renal failure
Venous trombosis, pulmonary embolism, gastric
ulcer
Paralytic Ileus & Decubitous ulcers
32.
PREVENTION
Infants bornto immune mothers acquire temporary immunity for
about five month, if mother had completed before 2wks of
delivery.
Vaccintion of ALL women in child bearing age is recommended
Use of safe delivery practices
Female education
Generally,TT vaccine given will produce protective antibodies
in 80-90% of the cases after the second dose,95-98% after the
3rd
dose
Fourth & fifth doses given will give protection for 10 & 20yrs
respectively.
33.
PROGNOSIS
MR <10%with ICU Rx & > 75% without it
Poor prognosis is associated with
IP < 7 DAYS
Period of onset < 3 days
Presence of autonomic dysfunction
Fever & frequent spasms
Good Prognosis is associated with
IP>7Days ,& period of onset >3days
Localized form
Occasional spasms, absence of fever
34.
COMMENTS
Mother didn’treceive any vaccination, home & risky delivery
No adequate treatment given;TAT, Muscle relaxants
Dose of Crystalline should have been 400,000IU/kg/d ; use
of Gentamycin good choice
Follow up should have included use of charts withV/S sheet,
type of resp., frequency of contraction, urine output, if
possible BP monitoring help us to guide management
& peak complications early.
Ideally management should be at NICU.
Maternal education!!!

















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)





![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)




