Download to read offline
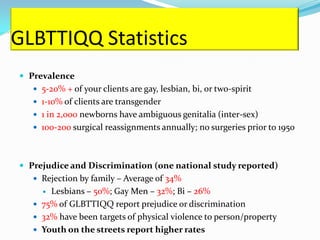
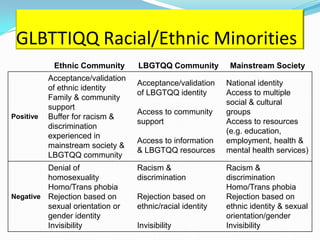




This document discusses providing culturally competent services to GLBTTIQQ (gay, lesbian, bisexual, transgender, transsexual, intersex, queer, and questioning) clients. It covers topics like understanding key terms, developing cultural competency, assessing for risks and needs of GLBTTIQQ clients, counseling approaches, working with families, making appropriate referrals, and advocating for GLBTTIQQ clients and employees. The goal is for organizations and professionals to be respectful, knowledgeable, and able to meet the needs of GLBTTIQQ individuals.














































































