Downloaded 48 times

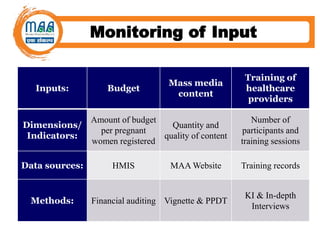
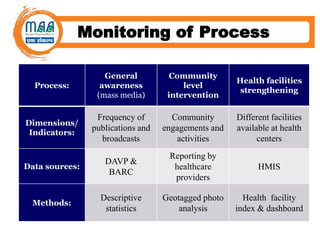
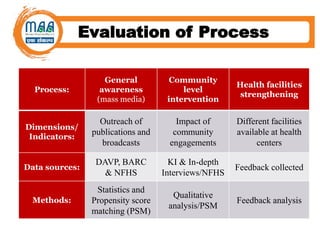
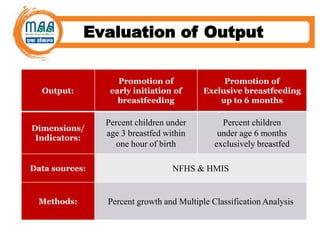
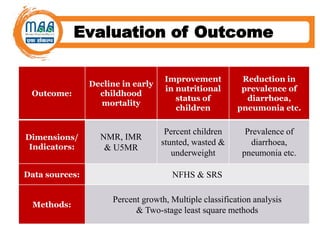
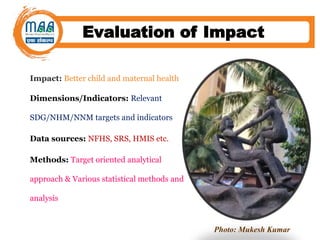
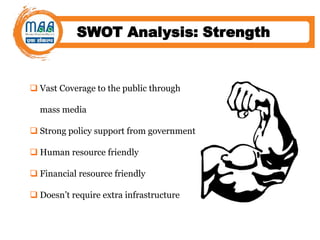
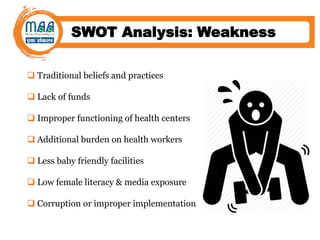


The document outlines the monitoring and evaluation framework for the Mothers' Absolute Affection (MAA) program initiated by the Government of India in 2016, aimed at promoting breastfeeding practices among pregnant and lactating mothers. It details the program's goals, objectives, implementation strategies, and expected outcomes, including declines in newborn and under-five mortality rates. The framework includes a logical approach to monitoring and evaluating the program's effectiveness through various metrics and indicators, alongside a SWOT analysis identifying strengths, weaknesses, opportunities, and threats.






























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)




