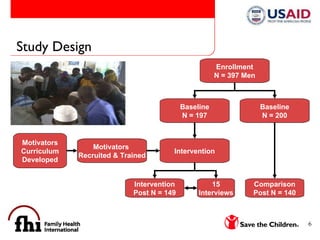
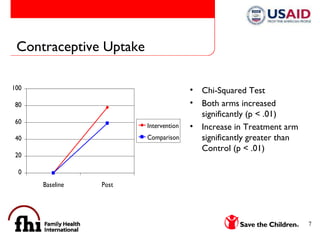
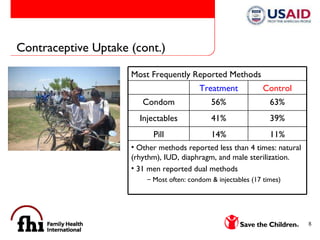
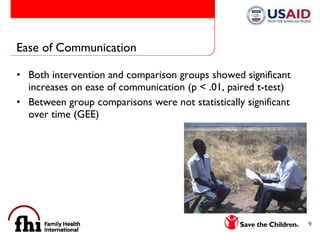
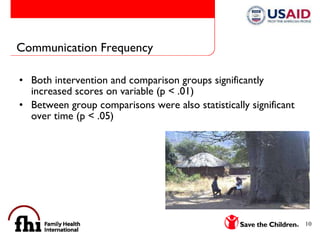
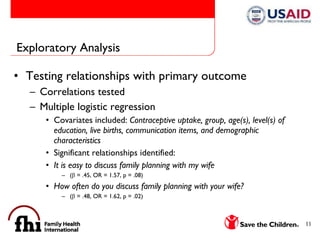
The document summarizes a study conducted in Malawi that tested the effectiveness of a male-focused family planning intervention at increasing contraceptive uptake. The intervention involved training male motivators who then visited married men over 8 months, providing information on family planning and teaching communication and motivation skills. The study found that contraceptive uptake increased significantly more in the intervention group compared to the control group. Improved communication between men and their wives about family planning was correlated with higher contraceptive use. The study demonstrates the potential for male-focused programs to promote family planning.

![Results: Qualitative Economic message received: “ Family planning is good and important because one is able take good care of the family with the limited resources available while a family that does not practice family planning has difficulties in taking care of the children since [financial] resources are very limited ...” Communication improved: “ Before the educator came to shed more light on this issue I was doing what I could, basing on guess work without even discussing with my wife. After the educator came I was able to discuss and communicate with my wife very well…”](https://image.slidesharecdn.com/shattuck6272-1260912372522-phpapp01/85/Malawi-Male-Motivators-12-320.jpg)




![Tb Education And Training Network Presentation0[1]](https://cdn.slidesharecdn.com/ss_thumbnails/tbeducationandtrainingnetworkpresentation01-1259588169189-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)