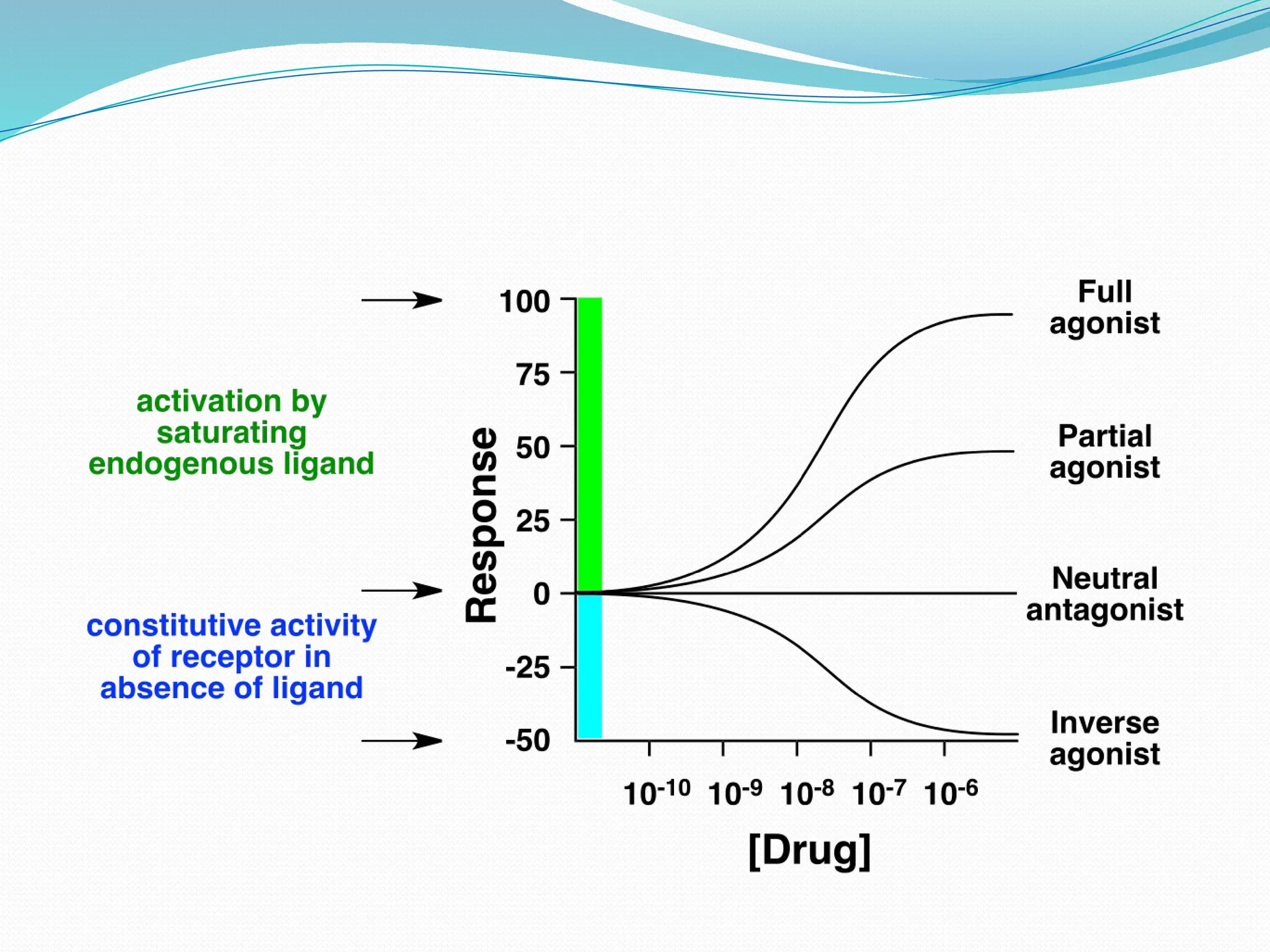
The document explains the definition and principles of pharmacology, specifically focusing on drug interactions with biological systems. It describes drug targets, including receptors, enzymes, and transporters, and distinguishes between agonists and antagonists in terms of their effects on receptors. Additionally, it addresses mechanisms of drug resistance and their implications for treatment effectiveness.