INTRODUCTION
Material is definedas “equipment, apparatus and
supplies used by an organization for the purpose of
rendering services”,
The basic objective of management is to optimize the
resources, i.e: Men, Money, Materials, Machines&
Minutes(time)
3.
INTRODUCTION
Lack of properattention to the material management in the
health system in the country has been a major problem in
effective implementation of various health programs
Man fails to realize the fact that material represents money
and also there is a lack of perception about the inter-
relatonship between money and the material
Non availability of drugs and materials supplies–
dissatisfaction among health personnel and also community
4.
DEFINITION
MM is ascientific technique which is concerned
with the planning, organizing and controlling the
flow of materials from their initial purchase through
internal operation to the distribution to the service
points
5.
BASIC FUNCTIONS OFMATERIAL MANAGEMENT
1. Effective management and supervision
2. Sound purchasing methods
3. An efficient purchase system
4. A simple inventory control programme
5. A result oriented requisition and distribution system
6. Written policies and procedures
7. A practical receiving programme: It denotes the need for
accountability and responsibility. For the best results, the
purchasing, receiving & paying of invoice should be done
by separate persons.
6.
AIM for MM
Tohave material in hand when needed
To pay the lowest possible price, consistent with quality
and value requirement
To minimize inventory investment
To operate efficiently
7.
•To gain economyin purchasing
•To satisfy the demand during period of
replenishment
•To carry reserve stock to avoid stock out
•To stabilize fluctuations in consumption
•To provide reasonable level of client services
PURPOSE OF MATERIAL
MANAGEMENT
8.
For delivery ofeffective health care services it is
necessary that-
Right material at right time at right place in right
quantity and of right quality should be made available
to perform the assigned activities in an effective and
efficient manner
Recurring expenditure of an average hospital –
60%---on salaries of employees
30-35%--- on materials
5-7% ---- on non material resources
9.
Stock: The goodskept on the premises of a
business or warehouse and available for sale or
distribution
Inventory–- total quantity of material available in
the store
Logistics–- defined as function of moving, storing
and distributing resources and goods
10.
Economy in MM
Purchase cost– actual cost of material
Carrying cost- cost of using or borrowing money
cost of storage space
cost of additional manpower
cost of obsolescence
cost of deterioration
cost of pilferage, breakage
Carrying cost may be 25-30% of the actual inventory cost
How to reduce it? Buy in small quantity.
But this increases PC
A point/ quantity at which both are minimum called economic order
quantity (EOQ)
11.
Shortage cost--- dealswith the cost of not having
a material. It would vary according to the nature of
an item
Ordering cost--- cost of placing an order to the
firm
12.
Primary
•Right price
•High inventoryturnover
•Low procurement & storage cost
•Continuity of supply
•Consistency in quality
•Cordial relationship with supplier
•Development of vendors
•Good information system
•Low storage cost
•Good records
Objective of material management
Advantages of MM
Improvedaccountability
Better coordination
Better performance
Analysis of data
Better team work
15.
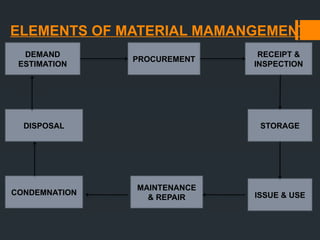
ELEMENTS OF MATERIALMAMANGEMENT
DEMAND
ESTIMATION
PROCUREMENT
DISPOSAL
CONDEMNATION
MAINTENANCE
& REPAIR ISSUE & USE
RECEIPT &
INSPECTION
STORAGE
16.
SELECTION AND DEMANDESTIMATION
Selection of items to be purchased need some basal
document, e.g., for medicines as per latest figure sixty
thousand formulation of drugs are manufactured and sold in
Indian market, while WHO says only three hundred odd
number of drugs are sufficient even for a tertiary hospital of
developing country.
Limited funds available are often ill spent on ineffective
duplication or unacceptable dangerous drugs.
It is therefore imperative to prepare a list of essential drugs
for a hospital & included in HOSPITAL FORMULARY.
17.
FORECEASTING OR ESTIMATINGDEMAND
Forecasting is the method of estimating demand based on time series
analysis of past while anticipating the future.
Demands for materials could be certain or predictable, and uncertain or
unpredictable.
Following guidelines:
Trends in consumption pattern during last 2-3 years.
Objective of the hospital.
Morbidity pattern of the community
The clienteles
Cyclic changes in epidemiological occurrence of disease.
Resources constraint.
Existing stock position.
18.
Methods of forecastingof demands in hospital
1. Last period demand–
2. The arithmetic average &
3. Moving average– it generates the next period’s
forecast by averaging the actual demands for the
last ‘n’ time periods
19.
PROCUREMENT
Process of acquiringsupplies
Three sources:
Purchase
Donations
Manufacturing
Objective of well procurement system:
Acquire needed supplies as inexpensively as possible.
Obtain supplies of high quality
Assure prompt, dependable delivery.
Distribute the procurement workload to avoid period of idleness &
overwork.
Optimize inventory management the scientific procurement procedures.
20.
PROCUREMENT
Methods of purchase:
TENDERBUYING
Open tender
Restricted tender
(selective)
Negotiated procurement
Direct procurement
RATE CONTRACT
Most important methods of procurement
of drugs as far as the govt. hospitals are
concerned. Under these contracts the
firms are asked to supply stores at
specified rates during period covered by
the contact.
DGS&D keeps a close watch.
Many state govt. & other organizations,
like ESI, have preferred to have their own
rate contract.
21.
RECEIPT AND INSPECTION
Suppliesoffered are received in the store.
The inspection policy should enunciate the sampling
procedure for inspection and this procedure must be followed.
At the point of delivery check each item physically and count
against supplier’s invoice
The lot thus picked up by a random sampling method should
be subjected to physical and chemical inspection. Thus any
discrepancy, problem or error in a specific transaction,
becomes evident during the receiving operation.
Carry out basic documents immediately i.e. day book or
inward good register
22.
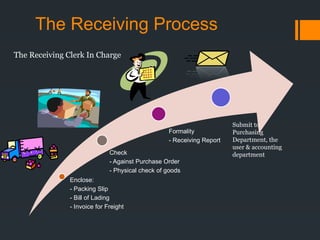
The Receiving Process
Enclose:
-Packing Slip
- Bill of Lading
- Invoice for Freight
Check
- Against Purchase Order
- Physical check of goods
Formality
- Receiving Report
Submit to
Purchasing
Department, the
user & accounting
department
The Receiving Clerk In Charge
23.
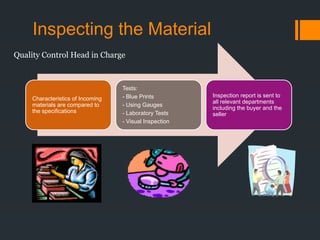
Inspecting the Material
Characteristicsof Incoming
materials are compared to
the specifications
Tests:
- Blue Prints
- Using Gauges
- Laboratory Tests
- Visual Inspection
Inspection report is sent to
all relevant departments
including the buyer and the
seller
Quality Control Head in Charge
24.
RECEIPT AND INSPECTION
Procedures:
Unloading& checking supplies
Unpacking & inspecting supplies
Goods received notes
Delivery of materials to the proper stocking locations
Receiving records shows–
- - which supplies are consistently late in their deliveries
-- which have the maximum number of rejects
---which deliver the greatest no. for split consignments
Any of these supplier is costly to the buyer
25.
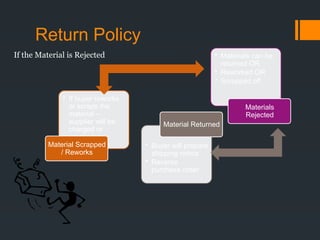
Return Policy
• Ifbuyer reworks
or scraps the
material –
supplier will be
charged or
credited
Material Scrapped
/ Reworks
• Buyer will prepare
shipping notice
• Reverse
purchase order
Material Returned
• Materials can be
returned OR
• Reworked OR
• Scrapped off
Materials
Rejected
If the Material is Rejected
26.
STORAGE
Medical store shouldbe accessible to supplies as well as
indenters.
Location of store will, therefore, be guided by the flow
activities of the store. Also, light, ventilation, cupboards,
shelves should be of adequate size.
Items received later from the supplies should be stored
behind similar items and the principle of FIFO should be
adopted.
Refrigerators or cold rooms are necessary.
Combustible and non-combustible– should be kept separate
Poisonous drugs & narcotics should be stored in locked
cupboards
Rodent free.
27.
STORAGE METHODS
The Two-Binsystem—stock of each item is physical
separated into two bins -–working bin and reserve bin
When working bin empty the store keeper changes to the
second bin and is alerted that new supplies are needed
Double shelf system – modification of two-bin system
This system works well only if the supply time is half the
purchasing interval
28.
ISSUE AND USE
Issue should be made after receiving written indents
Distribution system can be either by direct supply or through a sub store’
Push method (allocation system)
Pull methods (requisition system)
29.
Selective inventory control
LEAD TIME --It denotes the average duration of time between placing an
order to the supplier and receipt of materials in your medical stores
Internal lead time– duration between the moment at which some one is
aware of the need for the additional stock and order is placed
External lead time—taken by the supplier to supply the materials after it
receives the supply order from an org.
30.
Working stock– usedto satisfy the demand between
deliveries
Safety stock( Buffer stock)– exits to protect against stock
outs which would otherwise occur when either the
deliveries are delayed on the working stock is consumed at
an unexpectedly high rates
Reorder level-stock level at which a fresh order has to be
placed. It is equal to average consumption per day
multiplied by the lead time
31.
Inventory Control
If thematerial passes inspection
The receiving clerk usually prepares
a “Move Ticket”
Material is transferred to the User or
to the Storage Area
If transferred to stores – becomes
inventory
32.
Economy order quantity
Economyorder quantity– the quantity most economic to buy
EOQ = √2AC A=annual consumption in units
H C =cost of placing & receiving an order
p =purchase price per unit
H =holding cost per unit per year
Total annual cost
= (purchase cost) + (order cost) + (holding cost)
TC=AP +AC/Q +QH/2
33.
Suppose drugA priced at Rs 1000/- per box of 1000 tablets, with
1000 boxes being used per year. Placement of an order cost Rs
160/- and annual carrying cost after delivery is 20% of the purchase
price
√2CA/H = √2(160)A/200 = √1.6A = √1.6x 1000 = 40
Given the minimum cost order quantities, an order for 40 boxes
should be placed on 25 occasions during the year
Stock will vary between 0 to 40 boxes averaging 20
The ordering plus carrying cost will thus be 25(160)+ 20(200) = 8000
4000 + 4000
34.
If 100boxes ordered:
10(160) + 50(200)
1600 + 10000 = 11600
If 20 boxes are ordered:
50(160)+10(200)
8000+2000=10000
35.
Reorder Point
Quantity towhich inventory is allowed to drop before
replenishment order is made
Need to order EOQ at the Reorder Point:
ROP = D X LT
D = Demand rate per period
LT = lead time in periods
36.
SELECTIVE INVENTORY CONTROL
Effectivemanager should isolate those items that
require more precise control from those that do not
Items are classified into groups based on different
criteria
ABC analysis of drugs-- based on annual cost of the
items. Also known as Always Better Control
37.
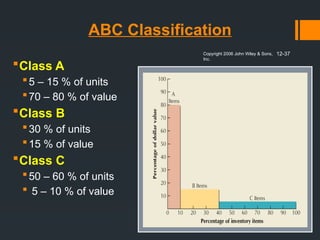
ABC Classification
Class A
5– 15 % of units
70 – 80 % of value
Class B
30 % of units
15 % of value
Class C
50 – 60 % of units
5 – 10 % of value
Copyright 2006 John Wiley & Sons,
Inc.
12-37
38.
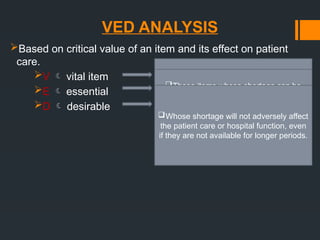
VED ANALYSIS
Based oncritical value of an item and its effect on patient
care.
V vital item
E essential
D desirable
Without which institution cannot
function.
Should always be present in sufficient
quantity and sufficient safety stock should
be maintained to ensure 100% availability.
Controlled by top manager levels.
Those items whose shortage can be
tolerated for short period only.
But if not available over a long period…
adversely affect patient care and hospital
functioning.
Controlled by middle manager level.
Whose shortage will not adversely affect
the patient care or hospital function, even
if they are not available for longer periods.
39.
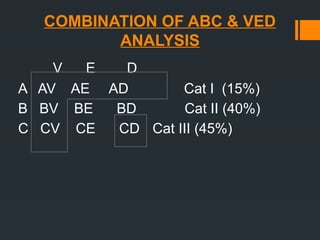
COMBINATION OF ABC& VED
ANALYSIS
V E D
A AV AE AD Cat I (15%)
B BV BE BD Cat II (40%)
C CV CE CD Cat III (45%)
40.
SDE ANALYSIS
Based onavailability position of items in market.
S scarce in market (imported drugs)
D difficult to obtain
E easily available
Used to avoid out of stock position of items.
FSN
Based on rate of consumption
F fast moving
S slow moving
N not moving
41.
Equipments Management
Equipments playa major role in a hospital.
Medical equipments aids the treating physician in providing
efficient health care in diagnostic and therapeutic areas and
make the patient stay comfortable
Effective management and efficient maintenance of health
care delivery and are vital for the smooth functioning of every
health facility from PHC to the most sophisticated hospital in
every country
42.
Problems- wide varietyof equipments at various level of
sophistication level but without adequate maintenance
support
Even less sophisticated equipments lead to high maintenance
cost by local agents
Lack of technically qualified manpower
A hostile environment
A developing country will seldom have about 50% of its
equipments in usable condition at a given time
43.
Before orderingan equipment hospital should ensure
Latest technology is being purchased
Full repair and maintenance facilities exist with a minimum of down time
Availability of post –warranty repair of reasonable cost
Purchased from reputed manufacture
Consumables are readily available
Operating cost should be low
44.
RECORDS NEEDED FORMAINTENANCE
HISTORY SHEET:
Identification data make model and date of purchase
Source of details of supplies and its spares
Purchase cost and detail of purchase procedure
Details of breakdowns and repair undertaken
Expenditure incurred on repair
LOG BOOK FOR EQUIPMENT:
Records for its maintenance should be kept, i.e., warranty period
& servicing/repair done, annual service contract, expenditure
incurred.
Details of preventive maintenance
Whether in working condition or not.
45.
RECORDS NEEDED FORMAINTENANCE
PERFORMANCE RECORD OF EQUIPMENT:
Essential to recommend for condemnation
Period since working
Level of utilization in terms of output
Periods when not working, with reasons
If beyond economic repair, a certificate from the
engineering unit should be procured.
46.
CONDEMNATION & DISPOSAL
Minimumcriteria to be followed for condemnation.
Non-functional and beyond economical repair
Non-functional and obsolete
Functional but obsolete
Functional but hazardous
Functional but no longer required
A CONDEMNATION COMMITTEE should be constituted for
assessing whether or not an equipment should be condemned
and disposed of based on the history sheet &
recommendations of the user department.
47.
CONDEMNATION & DISPOSAL
Thiscommittee should meet periodically at regular intervals, at
least twice an year.
However, for condemnation of costly hospital equipment, a
SPECIAL CONDEMNATION BOARD may be constituted as
per rule of the organization.
48.
CONDEMNATION & DISPOSAL
PROCEDURES:
Circulatewithin the hospitals, wards, OPD
Return to vendor if he is willing to accept
Sell to other hospitals
Sell to scrap dealers
Local destruction
By Auction: normally 10% of book price is accepted as
reserve price for auction
49.
CONCLUSION
Material management isan important management tool which
is very useful in getting the right quality & right quantity of
supplies at right time.
Provides good inventory control & helps in adopting sound
methods of condemnation & disposal, and therefore improves
the efficiency of the organization, whether it is Private,
Government, Small organization, Big organization or
Household. All these makes the working atmosphere healthy.
Even a common man must know the basics of material
management so that he can get the best of the available
resources and make it a habit to adopt the principles of
material management in all daily activities.