
Recommended
Recommended
More Related Content
Similar to Kunal Singh .Topic-4.Diseases of the larynx.ENT.GM20-148.pptx
Similar to Kunal Singh .Topic-4.Diseases of the larynx.ENT.GM20-148.pptx (20)
More from shiv847105
More from shiv847105 (8)
Recently uploaded
Recently uploaded (20)
Kunal Singh .Topic-4.Diseases of the larynx.ENT.GM20-148.pptx
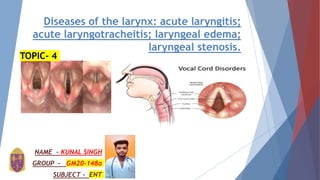
- 1. Diseases of the larynx: acute laryngitis; acute laryngotracheitis; laryngeal edema; laryngeal stenosis. NAME – KUNAL SINGH GROUP - GM20-148a SUBJECT - ENT TOPIC- 4
- 2. The larynx, or voice box, sits at the back of the throat, above the windpipe (trachea). It is supported by rings of cartilage, which form the bump of the Adam’s apple. The vocal cords are stretchy bands of tissue attached to the inside of the larynx. Air passing in and out of the lungs is pushed through these cords. Movements of the cartilage allow the vocal cords to contract or relax, which changes the pitch of sounds. Other body parts that influence the qualities of a person’s voice include the nose, mouth, tongue, jaw and throat. The larynx also contains an important flap or valve called the epiglottis, which covers the trachea whenever we swallow to prevent foods or liquid entering the lungs. Various infections and disorders, such as cancer, can affect the larynx. The usual symptom is hoarseness. INTRODUCTION
- 3. Diseases of the Larynx This is an example of a normal larynx. The true vocal folds are pearly white, they meet in the midline on phonation, and the surrounding structures are light pink. As you view the following examples of diseases of the larynx, you can compare them to this example. •The larynx (voice box) contains the vocal cords, which allow speech. •Disorders of the larynx include laryngitis, croup, growths and cancer. •A common irritation to the larynx is voice abuse, which includes • screaming, singing or shouting too much.
- 5. Acute laryngitis Acute laryngitis is characterized by inflammation and congestion of the larynx in the early stages. This can encompass the supraglottic, glottic, or subglottic larynx (or any combination thereof), depending on the inciting organism. As the healing stage begins, white blood cells arrive at the site of infection to remove the pathogens. This process enhances vocal cord edema and affects vibration adversely, changing the amplitude, magnitude, and frequency of the normal vocal fold dynamic. As the edema progresses, the phonation threshold pressure can increase. The generation of adequate phonation pressure becomes more difficult, and the patient develops phonatory changes both as a result of the changing fluid-wave dynamics of the inflamed and edematous tissue, but also as a result of both conscious and unconscious adaptation to attempt to mitigate these altered tissue dynamics.
- 6. Etiology The etiology of acute laryngitis can be classified as either infectious or non-infectious. The infectious form is more common and usually follows an upper respiratory tract infection. Viral agents such as rhinovirus, parainfluenza virus, respiratory syncytial virus, coronavirus, adenovirus, and influenza are all potential etiologic agents (listed in roughly descending order of frequency). It is possible for bacterial superinfection to occur in the setting of viral laryngitis, this classically occurs approximately seven days after symptoms begin. The most commonly encountered bacterial organisms are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis, in that order. Exanthematous febrile illnesses such as measles, chickenpox, and whooping cough are also associated with acute laryngitis symptoms, so it is prudent to obtain an accurate immunization history. Laryngitis caused by fungal infection is very rare in immunocompetent individuals, and more often presents as chronic laryngitis in the immunocompromised or in patients using inhaled steroid medications.
- 7. Epidemiology Acute laryngitis can affect patients of any age, though is more common in the adult population, usually affecting individuals aged 18 to 40, though it may be seen in children as young as three. Isolated voice symptoms in children younger than three should prompt a more thorough workup for additional pathology including vocal cord paralysis, GERD, and neurodevelopmental conditions. Accurate incidence measurements of acute laryngitis remain difficult to elucidate as this condition remains under-reported, with many patients appropriately not seeking medical care for this often self-limited condition
- 8. Evaluation Diagnosis is usually made via a very thorough history and physical examination. Formal voice analysis and fiberoptic laryngoscopy can be used to confirm the diagnosis in cases that are refractory to treatment or otherwise convoluted. Stroboscopy may be relatively normal or may reveal asymmetry, aperiodicity, and reduced mucosal wave patterns . Further imaging or laboratory studies are not required unless an atypical pathogen or neoplasm are suspected. Rarely, if the patient has exudate in the oropharynx or vocal cords, culture may be indicated.
- 9. Treatment / Management Treatment is often supportive in nature and depends on the severity of laryngitis. •Voice rest: This is the single most important factor. Use of voice during laryngitis results in incomplete or delayed recovery. Complete voice rest is recommended although it is almost impossible to achieve. If the patient needs to speak, the patient should be instructed to use a "confidential voice;" that is, a normal phonatory voice at low volume without whispering or projecting.l •Steam Inhalation: Inhaling humidified air enhances moisture of the upper airway and helps in the removal of secretions and exudates. •Avoidance of irritants: Smoking and alcohol should be avoided. Smoking delays prompt resolution of the disease process. •Dietary modification: dietary restriction is recommended for patients with gastroesophageal reflux disease. This includes avoiding caffeinated drinks, spicy food items, fatty food, chocolate, peppermint. Another important lifestyle modification is the avoidance of late meals. The patient should have meals at least 3 hours before sleeping. The patient should drink plenty of water. These dietary measures have been shown to be effective in classic GERD, though their efficacy in LPR is disputed, they are often still employed. •Medications: Antibiotics prescription for an otherwise healthy patient with acute laryngitis is currently unsupported; however for high-risk patients and patients with severe symptoms antibiotics may be given. Some authors recommend narrow-spectrum antibiotics only in the presence of identifiable gram stain and culture.
- 10. Differential Diagnosis This includes: •Spasmodic dysphonia •Reflux laryngitis •Chronic allergic laryngitis •Epiglottitis •Neoplasm Prognosis As this is often a self-limiting condition, it carries a good prognosis. If the patient completes the recommended therapy, the prognosis for recovery to a premorbid level of phonation is excellent. If vocal maladaptations have occurred, a course of speech therapy can resolve these problems.
- 11. Acute laryngotracheitis laryngotracheitis (ILT) is a respiratory disease almost exclusively of chickens. Infections in turkeys and pheasants have been reported, but surveys have yielded no wild bird reservoir or other domestic poultry reservoir (Cranshaw and Boycott, 1982). Based on this and the knowledge that ILT apparently exhibits little antigenic heterogeneity, it has been proposed that through proper husbandry practices and appropriate vaccination techniques the disease could be eliminated from commercial poultry (Bagust and Johnson, 1998). The virus is a member of the Alphaherpesvirinae subfamily and is identified taxonomically as gallid herpesvirus I. The disease is almost exclusively respiratory, with no systemic involvement.
- 12. Acute laryngotracheitis is an inflammation of both the larynx (voice box) and the trachea (windpipe). It is often caused by a viral infection, such as the common cold or influenza, and it can result in a range of symptoms, including: Hoarseness: A hoarse or raspy voice is a common symptom. Cough: Laryngotracheitis can lead to a persistent, dry cough. Sore Throat: Individuals may experience a sore or scratchy throat. Difficulty Breathing: Swelling in the airways can cause breathing difficulties, particularly in children. Fever: Some cases may be associated with a mild fever. Wheezing: Wheezing, a high-pitched whistling sound when breathing, can occur in severe cases. Acute laryngotracheitis
- 19. laryngeal edema
- 20. Laryngeal edema is the swelling of the larynx (voice box) due to an accumulation of fluid. It can be caused by various factors, such as infections, allergic reactions, trauma, or underlying medical conditions. Laryngeal edema can be a medical emergency because it can obstruct the airway and lead to breathing difficulties. Laryngeal edema
- 25. laryngeal stenosis Laryngeal stenosis refers to a narrowing of the larynx (voice box) or the airway within the larynx. This narrowing can occur due to various factors, including scarring, inflammation, injury, or congenital abnormalities. Laryngeal stenosis can lead to breathing difficulties and voice changes.
- 28. Stridor: High-pitched, noisy breathing during inhalation. Shortness of Breath: Difficulty breathing, especially during physical activity . Hoarseness: Changes in the voice, often becoming hoarse. Cough: Chronic cough due to irritation. SYMPTOMS
- 32. Thankyou for your Attention NAME – KUNAL SINGH GROUP - GM20-148a SUBJECT - ENT