• A 49-year-oldmale farm worker presented to the hospital with a 4-day history of dizziness
• fatigue
• chest tightness,
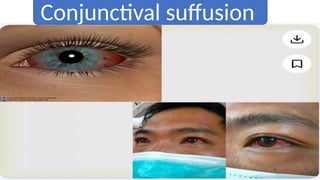
• cough, chills, fever, conjunctival congestion
• myalgia.
• He also had a history of haemoptysis, which resulted in emergency admission. He had no
significant medical history.
• Upon admission to our hospital, the patient was conscious with a body temperature of
38.7°C,
• pulse rate of 106 beats/minute,
• respiration rate of 32 breaths/minute,
• and blood pressure of 96/62 mmHg.
• He also had shortness of breath and tachycardia.
Clinical Case
4.
• Haemoglobin levelof 10.7 g/L
• thrombocytopenia platelet count of 62,000
• inflammation as indicated by a C-reactive protein level of 138.2 mg/L
• and liver dysfunction as shown by an aspartate aminotransferase
level of 62 U/L
• alanine aminotransferase level of 70 U/L
• Urinalysis revealed haematuria, mild proteinuria, and leukocytes in
the urine.
• During the night of admission, the patient’s condition deteriorated
and he developed massive haemoptysis, dyspnoea, and cold
extremities.
5.
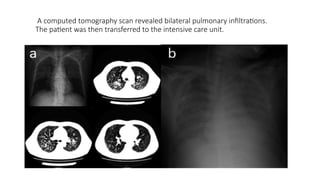
A computed tomographyscan revealed bilateral pulmonary infiltrations.
The patient was then transferred to the intensive care unit.
6.
• In theintensive care unit, he was placed on mechanical ventilation and treated with
several doses of a fluid bolus (normal saline),
• broad-spectrum antibiotics
• haemostatics
• blood transfusion (red blood cell suspension and platelets) for 3 days. However, this
treatment was ineffective.
• On the third day of admission, he started desaturating due to continuous massive
pulmonary haemorrhage despite the mechanical ventilation.
• He developed multiple organ dysfunction syndrome, including liver failure, renal failure,
and myocardial depression.
• His aspartate aminotransferase, creatinine, CK-MB, and PaO2/FiO2 ratio were 4660 U/L,
247 µmol/L, 356 IU/L, and 70, respectively. Veno-venous extracorporeal membrane
oxygenation and continuous renal replacement therapy were initiated
• . Under extracorporeal life support (ECLS), his blood pressure was 130–100/50–30 mmHg
(with administration of norepinephrine at 2 µg/kg/minute)
• His arterial oxygen saturation was 88% to 96%. Meanwhile, his microcirculation was
suboptimal as indicated by anuria
7.
• hyperlactic acidaemia
•His finger pulse oxygenation readings could not be obtained.
• On the fourth day of admission, fibreoptic bronchoscopy revealed diffuse haemorrhage in the mucosa of
the bronchi and bronchioles.
• We sequenced the specimens collected from the airway and alveolar lavage fluid using next-generation
gene sequencing (NGS).
• The next day, the DNA of Leptospira interrogans was detected in the bronchoalveolar lavage fluid by NGS
(shotgun sequencing).
• With the patient’s possible history of contact with contaminated water and the DNA sequence
of Leptospira detected in his bronchoalveolar lavage fluid, pulmonary haemorrhagic leptospirosis was
considered, and the patient was treated with intravenous injection of penicillin every 6 hours.
• Unfortunately, despite aggressive treatment to control the pulmonary haemorrhage, the massive
haemoptysis persisted.
• On the fifth day of admission, the patient’s haemoglobin level dropped from 107 to 65 g/L, his platelet
count dropped from 62 to 43 × 109
/L
• his fibrinogen level dropped from 7.70 to 0.76 mg/dL because of the massive haemoptysis, regardless of
the blood products that had been administered during the previous 3 days (46.5 U red blood cell
suspension, 40 U platelets
• 3980 mL fresh frozen plasma, and 20 U cryoprecipitate. On day 6 of admission, the patient died of
haemorrhagic shock caused by refractory pulmonary haemorrhage and irreversible multiple organ failure.
•Zoonotic disease
•Caused byspirochete Leptospira.
•Historically known as Weil’s disease.
•Described in 1885 by Adolf weil with clinical hall marks of
Splenomegaly
Jaundice
Nephritis
INTRODUCTION
11.
One of theemerging infectious disease
since the late 1990
Recent large out breaks in several Asian ,
Central and South American countries
Becoming an important public health
problem , yet it continues to be under
recognized
12.
Genus Leptospira ,order Spirochetales ,
family Leptospiraceae.
Can live both in animals and free in the
environment (both pathogenic and
saprophytic).
Around 250 serovars from 20 species cause
disease in humans and animals.
Organism
13.
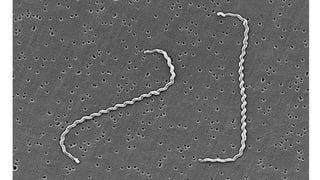
All species aremorphologically identical
Tightly and regularly coiled with hooked
ends.
Highly motile along the longitudinal axis.
Gram Negative and Aerobic
Morphology
15.
Not seen bydirect light microscopy
Dark field or phase contrast microscopy must be used
In tissues
Silver impregnation(Warthin starry staining)
Immunohistochemistry or
Immunoflourescene microscopy
Isolation difficult
16.
Zoonotic disease
No humanto human transmission
Most important sources are rats , dogs , cattle and pigs.
The most common culture medium for leptospira is Ellinghausen
McCullough – johnson – Harris(EMJH)medium
Noble agar
Fletchers medium
Epidemiology
17.
Domestic animals :Temporary carrier
Rodents : Permanent carrier
Rodents are therefore considered as the
major reservoir of infection.
RAT(Rattus norvegicus and Rattus rattus )
Associated L.interrogans serovars
Icterohaemorrhagic and copenhageni are
mostly associated with Weil’s disease.
18.
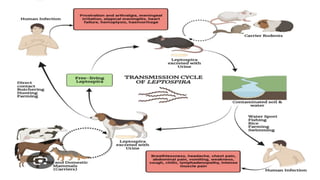
Transmitted through contactwith infected animal urine and other
excreta (Eg Placenta).
Contact may be
Direct or
Indirect through surface water or moist soil.
• Seasonal rainsand flooding are the most important factors causing
epidemics
Endemic disease is facilitated by
Tropical humid environment
Poor sanitation
Rodent and dog population
22.
Sporadic diseaseis associated with
Occupation : Veterinary , sewer and slaughter house workers.
Poor hygiene areas e.g. Slums
Adventure travel
Military training
24.
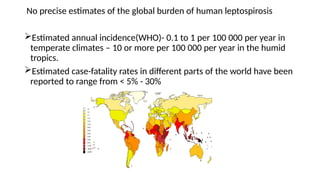
No precise estimatesof the global burden of human leptospirosis
Estimated annual incidence(WHO)- 0.1 to 1 per 100 000 per year in
temperate climates – 10 or more per 100 000 per year in the humid
tropics.
Estimated case-fatality rates in different parts of the world have been
reported to range from < 5% - 30%
25.
Considered a rarezoonotic disease in India with only sporadic cases
being recorded
Since 1980’s the disease has been reported from various states during
monsoon months in mini epidemic proportions.
Indian perspective
26.
The disease isendemic in
Kerala
Tamil Nadu
Gujarat
Andamans
Karnataka
Maharashtra
It has also been reported from Andhra pradesh , Orissa , West
Bengal , Uttar Pradesh , Delhi & puducherry
27.
Leptospirosis has beenunder – reported and under – diagnosed from
India due to
Lack of awareness of the disease and
Lack of appropriate laboratory diagnostic facilities in most parts of
the country .
31.
Clinical expression canbe
Sub clinical infection 90 %
Undifferentiated febrile ill ness
Weil’s disease 10%
Severe pulmonary haemorrhagic syndrome
Incubation period 2-30 days (Average 5-14 days).
Clinical Features
32.
Classically described asBiphasic
Acute phase :
3- 10 days
Leptospiraemia : blood culture may be positive
This phase responds to antibiotics
Immune phase:
This phase less responds to antibiotics
Isolation from Urine
This phase is mediated by antibodies and immunocomplexes which
damages the tissues.(cytokine storm)
It occurs in10% of leptospira cases.
The most severe form of Leptospirosis
Monophasic and fluminant
Variable combinations of jaundice , Acute kidney injury , Hypotension
and Haemorrhage.
Pulmonary haemorrhage(50% - 70% mortality)
Multisystem involvement occurs
Weil’s Disease
38.
Presents with jaundice
Itcauses acute hepatitis
LFT-TB ,SGOT,SGPT are markedly elevated .
Liver can be enlarged and tender
Splenomegaly in minority of patients
In severe cases may progress to acute liver failure.
MARS (molecular adsorbent recirculating system).
( Liver dialysis)
Liver involvement
39.
Can manifest afterseveral days of illness
Can be oliguric /Non oliguric
Dyselectrolytemia is common : hypokalemia , hyponatremia and
hypomagnesemia is non –oliguric disease
Hypotension may cause tubular necrosis and oliguria
In the first week acute tubular necrosis occur in acute phase.
Acute interstitial nephritis occur in the immune phase of illness.
Patient may require haemodialysis or CRRT.
Kidney involvement
40.
s
• Leptospirosis inpregnancy is a severe zoonotic disease that can lead to severe
complications for both mother and the foetus including miscarriage , still birth
and fetal death.
• It crosses placenta
• Maternal adverse outcomes
Subclinical,undifferentiated fever ,weil’s disease, severe pulmonary
haemorrhagic syndrome, ARDS ,MODS and maternal death
Foetus ------It causes abortion, stillbirth , IUDR, small for gestational age ,foetal
death.
The complications are more in second trimester than third trimester
Leptospirosis in Pregnancy
41.
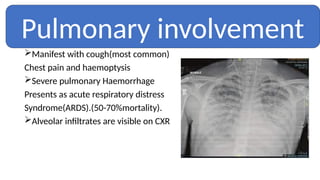
Manifest with cough(mostcommon)
Chest pain and haemoptysis
Severe pulmonary Haemorrhage
Presents as acute respiratory distress
Syndrome(ARDS).(50-70%mortality).
Alveolar infiltrates are visible on CXR
Pulmonary involvement
42.
Cardiac
Myocarditis
Neurological
Aseptic meningitis
Hypo orareflexia
Eyes:
Uveitis
Skeletal muscles:
Severe myalgia of calves and abdominal muscles , rhabdomyolysis
Cholecystitis
Pancreatitis (can cause hypo / hyperglycemia)
Other manifestations
43.
High index ofsuspicion is critical in a setting of
An appropriate exposure history
Infection’s protean manifestations
Biochemical , Hematological and urinalysis may suggest but are not
specific for diagnosis.
Diagnosis
44.
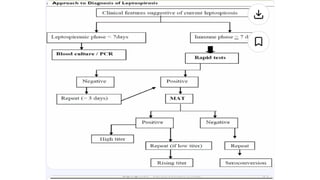
The disease isusually diagnosed by –
Detecting antibodies using various serological tests
Culturing the bacteria from blood , CSF ,urine and tissues
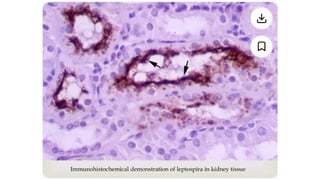
Demonstrating the presence of leptospires in tissues using antibodies labelled
with fluorescent markers
Polymerase chain reaction
Immuno staining
Culture take many weeks and can not guide clinical care
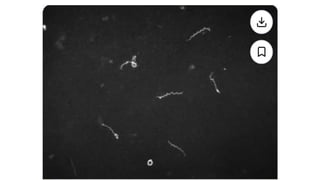
Dark field microscopy of blood /urine not recommended
47.
Microscopic agglutination test(MAT) is the gold standard : sensitivity
92% Specificity 95%
MAT has a very limited availability
Serological tests
48.
When patients havea high pretest probability : a single antibody titer
>1:200 is considered strong evidence infection
In regions where leptospirosis transmission and subclinical disease are
common , higher titres are generally required
MAT is generally negative in the first 7-10days after the onset of infection
Paired acute – and convalescent – phase serum samples are preferred to
document sero conversion or a four fold rise in titer
50.
Genus specific orrapid test include
ELISA
Macroscopic slide agglutination test (MSAT)
Latex agglutination test
Dipstick Tests (Lepto dipstick , Lepto tek lateral flow)
Lepto Tek Dri –Dor test
Indirect hemagglutination
51.
Leptospires can becultured from blood and csf during first 7-10 days
URINE CULTURE USEFUL BEGINNING IN THE 2ND
WEEK
May take 2 -4 weeks to be positive
Urine cultures can remain positive for many months / years despite
therapy
Isolation
Prompt initiating ofantibiotic therapy shortens the course and
prevents progression
Mild Leptospirosis resolves with out any tretment
Treatment
57.
Renal involvement mayrequire haemodialysis
Hypotension can be managed by fluids and vasopressors
Severe disease should be treated empirically with broad spectrum
antibiotics before confirmation
Severe pulmonary haemorrhagic syndrome should be immediately
incubated and mechanically ventilated.
In severe cases VV-ECMO ,plasmapheresis ,iv methylprednisolone can be
used.
58.
Advanced age ,pulmonary involvement , elevated creatinine ,
oliguria and thrombocytopenia indicate poor prognosis
Severe liver dysfunction is associated with poor prognosis.
In many cases no permanent sequelae or progressive organ
dysfunction after resolution
Prognosis
59.
No vaccine availablecurrently for humans.
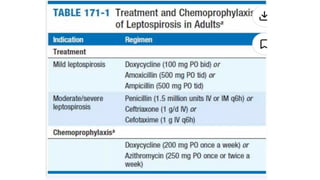
Short term antibiotic prophylaxis can be used for well – defined
exposures
Doxycycline 100mg or Azithromycin 250 mg once a week may be used
Avoid contaminated water
Wear protective gear
Control Rodents
Wash skin immediately
Drink safe water
Vaccinate pets
Prevention
61.
• Caused byLeptospira bacteria, often found in water contaminated with urine from
infected animals.
• Common in tropical and subtropical regions, especially after floods.Symptoms range
from mild flu-like illness to severe complications (e.g., kidney/liver failure, Weil’s
disease).
• Wear protective clothing and avoid swimming or wading in potentially contaminated
water.
• Antibiotics are effective, especially if started early.
Summary
62.
Adequate historyof exposure is most important in diagnosis
Possibility of leptospirosis to be kept in d/d of all icteric illness
Prompt treatment can prevent life threatening complications
Health education and awareness for prevention
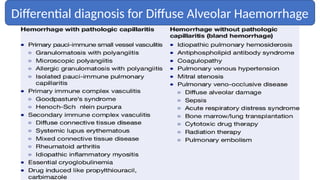
Leptospirosis should be considered in the differential diagnosis of
diffuse alveolar haemorrhage
Take home message