Download to read offline




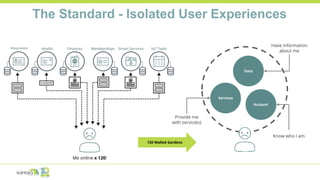


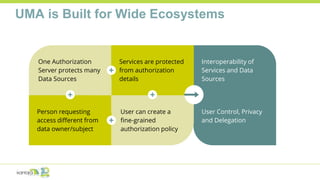
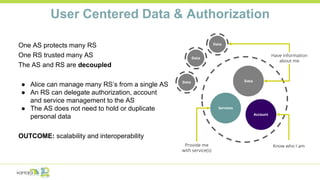
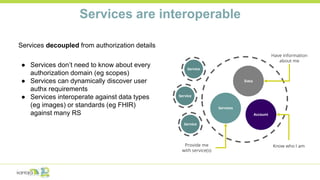
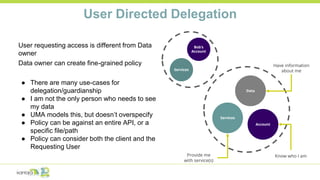
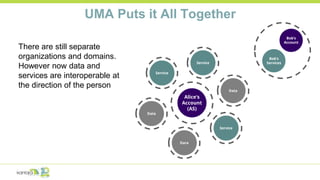
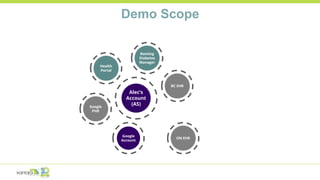



This document summarizes a presentation on how the User Managed Access (UMA) standard addresses challenges in health information interoperability and user control. It discusses how current health systems have data silos and lack of user access to their own health records. UMA allows for interoperability across services/data sources through a centralized authorization server. It enables user-directed delegation so others can access data on a user's behalf. Case studies demonstrate implementations like Trustee that use UMA to create a self-sovereign universal health record. Another case study discusses Ontario's FPX which uses UMA and standards for identity, authentication, and access in health care.







![Health delivery information system [HDIS] MVP](https://cdn.slidesharecdn.com/ss_thumbnails/healthdeliveryinformationsystemhdismvp-210419073440-thumbnail.jpg?width=640&height=640&fit=bounds)













![Himss Revenue Cycle Task Force Panel Presentation[1]](https://cdn.slidesharecdn.com/ss_thumbnails/himssrevenuecycletaskforcepanelpresentation1-13003099873448-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
































































