Downloaded 13 times


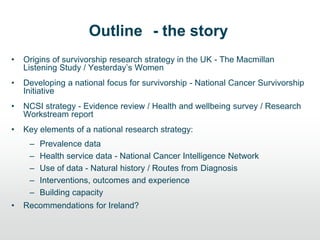
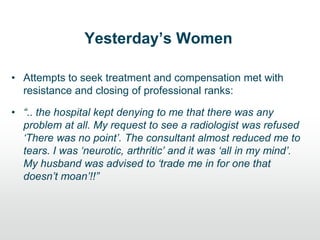
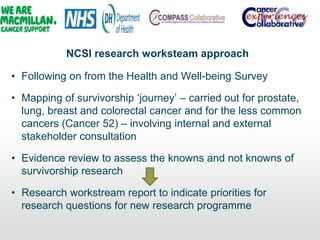
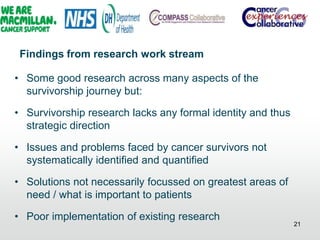
![Rank Key theme Total rank score
[Possible
Range: 1 – 102]
No. consultation
groups in which
topic received at
least one vote
N=17
1 Impact on life, how to live with cancer and related
support issues
68 13
2 Risk factors and causes 58 12
3 Early detection and prevention 48 9
4 Research into general information needs (on
cancer, treatment, research and access to)
34 11
5 Use and effectiveness of complementary and
alternative therapies
30 7
6 General education of public about cancer 24 5
7 Research into different cancer and patient types 23 7
7 Research on treatment (curative treatment,
treatment types and improvements)
23 5
7 Experiences and management of side effects 23 7
8 Organisation and funding of health and social
care services
21 6
9 Coordination, impact and funding of research 19 4
10 Research into recurrence 11 3
11 General communication issues involving all
parties
10 3
12 Accessing patients‟ views about cancer, services
and research
9 2
13 Health and safety in the hospital 1 1
Corner, J. et al., (2007) The research priorities of patients attending UK cancer treatment centres: Findings from a
modified nominal group study. British Journal of Cancer, 96(6), 875-881.](https://image.slidesharecdn.com/jimelliottpresentation-130930091029-phpapp01/85/Developing-a-national-strategy-for-research-into-cancer-survivorship-in-the-UK-Dr-Jim-Elliott-UK-NCRI-5-320.jpg)
![A national focus for survivorship
• National Cancer Survivorship Initiative (NCSI)
• Joint initiative by Department of Health, Macmillan Cancer
Support and NHS Improvement to address the long term
[unmet] needs of people living with and beyond cancer
• 2010 Vision to ensure that survivors get the care and
support they need to lead as healthy and active a life as
possible, for as long as possible](https://image.slidesharecdn.com/jimelliottpresentation-130930091029-phpapp01/85/Developing-a-national-strategy-for-research-into-cancer-survivorship-in-the-UK-Dr-Jim-Elliott-UK-NCRI-9-320.jpg)
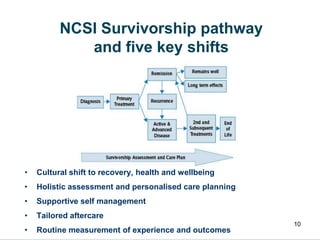

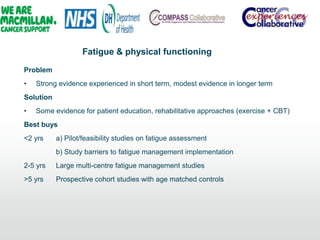
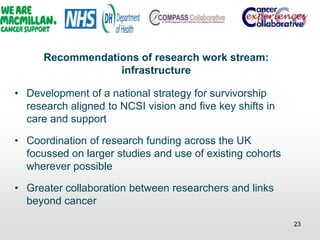
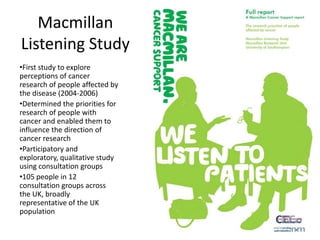
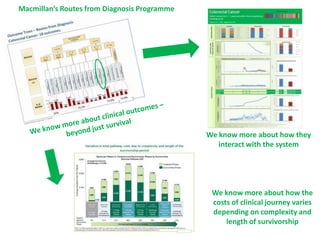
![The cancer care pathway
Diagnosis &
Treatment
Recovery and
adjustment
Early
monitoring
End of life care
[Year 1 deaths]
Progressive
illness
Later
monitoring
Newly
diagnosed –
assumed need
of acute
sector care
Surviving the
first year –
assumed need
of rehabilitation
Up to 5 and 10
years from
diagnosis –
designated as
‘early
monitoring’
Incurable
disease but not
in last year of
life
End of life care
in last year
Beyond 10
years from
diagnosis –
designated
‘later
monitoring’
Transition Points](https://image.slidesharecdn.com/jimelliottpresentation-130930091029-phpapp01/85/Developing-a-national-strategy-for-research-into-cancer-survivorship-in-the-UK-Dr-Jim-Elliott-UK-NCRI-27-320.jpg)

![Interventions
• Still a need for trials and other well designed
studies to develop and evaluate interventions for
specific conditions
• Currently left to individual research teams [still] in
absence of collaborative national research strategy
• Build on and update NCSI evidence review
• Must not forget social consequences too](https://image.slidesharecdn.com/jimelliottpresentation-130930091029-phpapp01/85/Developing-a-national-strategy-for-research-into-cancer-survivorship-in-the-UK-Dr-Jim-Elliott-UK-NCRI-34-320.jpg)

![Building capacity
• Collaboration key to avoid isolation
• Need for fellowships and career structure
[still] to build critical mass and attract
researchers to the field](https://image.slidesharecdn.com/jimelliottpresentation-130930091029-phpapp01/85/Developing-a-national-strategy-for-research-into-cancer-survivorship-in-the-UK-Dr-Jim-Elliott-UK-NCRI-37-320.jpg)


The document outlines the development of a national strategy for cancer survivorship research in the UK, emphasizing the importance of understanding the long-term needs of cancer survivors. It discusses various research initiatives, findings from surveys about survivor challenges, and the need for greater collaboration and data collection. The report also highlights key recommendations for improving survivorship care and research, particularly relevant for Ireland.






































































































