Download to read offline

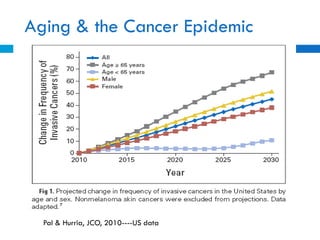


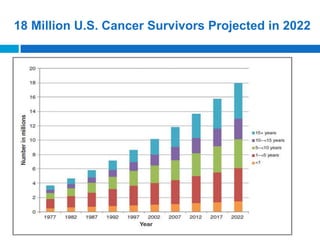


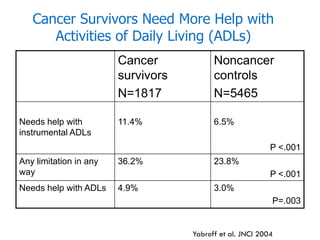

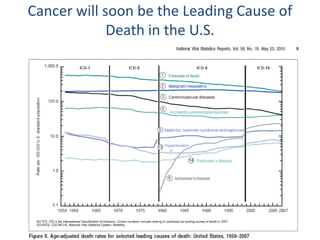

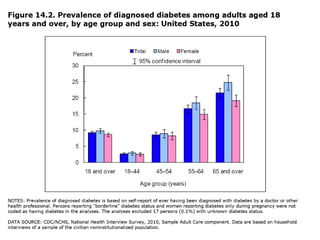



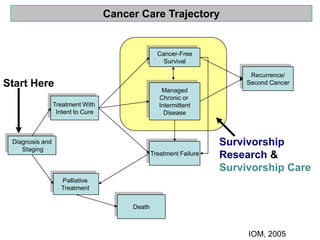





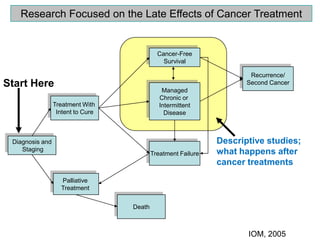

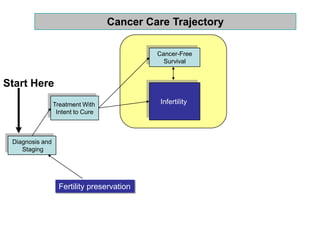
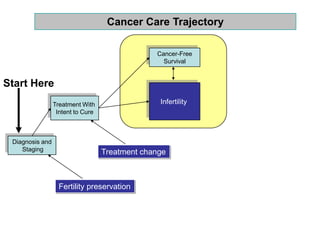



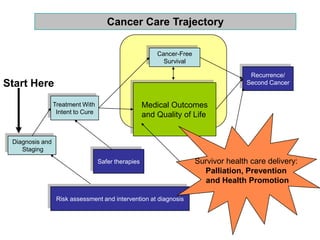

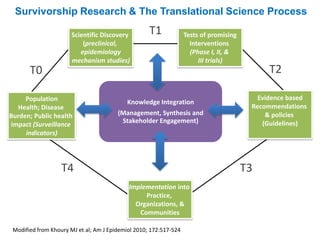

The document summarizes challenges and opportunities for developing a cancer survivorship research agenda. It notes that the aging population will lead to a large increase in cancer cases and survivors in coming decades. Cancer survivors often face significant physical and mental health issues. More research is needed to understand late effects of treatments and better deliver palliative care, prevention, and health promotion to survivors. Opportunities exist to form interdisciplinary teams, study symptoms and comorbidities, develop safer therapies, and test new models of survivor care. Where to start depends on available populations and expertise. Translational research integrating population health and scientific discovery is key.























































































